INTRODUCTION
There is indisputable evidence that tobacco use is a substantial public health concern with considerable economic ramifications1-4. The World Health Organization reports that global smoking-related diseases cost US$1911 billion per year and that by 2030 more than 8 million people will die annually from tobacco use5,6. The regions of the World do not share equally the burden of tobacco-related disease and death. For instance, 40% of the costs of smoking are currently borne by developing nations and it is projected that by 2030 more than 80% of premature deaths due to tobacco will occur in low-and middle-income countries5-7. Among developing nations, tobacco use in African countries has received little attention given the perceived low rate of use and the critical need for more interventions for both infectious and non-infectious diseases. However, improved economic growth and health has resulted in Africa becoming a prime target for market growth by multinational tobacco companies and rates of use are rising8.
Uganda ratified the WHO Framework for Convention of Tobacco Control (FCTC) in 20079. As a result, Uganda enacted the Tobacco Control Act in 2015, which prohibits smoking in public places, calls for a comprehensive ban on both direct and indirect tobacco advertising and graphic health warnings covering 65% of both principal display areas of tobacco packaging, as well as a ban on misleading labeling including terms such as ‘light’ and ‘low tar’ and other such signs. Tobacco policy requires prominent and clear display of no smoking signage in local languages including Swahili and English, the two official languages in Uganda. In a similar vein, the provisions of smoke-free laws are enforced by authorized officials including police officers, public health officers, environmental inspectors, custom officers and any other person or group of persons appointed by the Minister of Health10.
Despite passage of tobacco control laws in Uganda, the process of implementation has not yet been fully aligned with WHO guidelines11,12. At present, approximately 5.3% of Ugandans smoke cigarettes and 7.9% consume tobacco, which costs Uganda nearly US$40.8 million due to smoking related diseases and 13500 premature deaths annually1. In addition, there are subgroups within Uganda that have high rates of tobacco use, such as the military1. Police officers are required to maintain readiness and optimum levels of performance as they operate in numerous environments, ranging from urban locations to remote theaters of operation. Police officers also, unfortunately, belong to the category of professions whose occupational culture increases vulnerability to smoking cigarettes13-16. Studies conducted in developed countries found that tobacco use is higher among police officers compared to the general population. In the US, prevalence of cigarette smoking is 16.7% among police officers versus 15.5% in the general population, while in Australia it is 19.4% compared to 14.5% nationally17,18. As smokers, police officers soften, become sick, experience increased absenteeism and presenteeism, retire early, and load insurance premiums to nearly US$170 billion each year19. Given the police’s role in law enforcement, much is at stake as public security is compromised by tobacco use and has led to several researchers suggesting smoke-free policies in police departments19,20.
The Ugandan Police Force (UPF) is a large employer with nearly 44601 active personnel in its service who are saddled with the constitutional roles of law enforcement. The UPF consists mainly of GGD (guard and general patrol duties) and special support forces (SF) units. The SF unit comprises traffic, special branch, criminal investigations, and administration. The ratio of police officers to population in Uganda is approximately 1 officer per 1000 inhabitants, compared to the United Nations’ recommended ratio of 1 officer to 500 people21. As in upper income countries, police in Uganda are likely to be at high risk for tobacco use. For instance, in Uganda men have approximately triple the rate of tobacco use found among women (11.6% vs 4.6%)1. Given that the majority of police officers are males they are at higher risk of use. Tobacco use among Ugandan police officers would have consequences beyond their profession given that they often serve as role models for the nation’s youth and are required to enforce the tobacco law.
To date, no research has ever been conducted on tobacco use in the UPF. Data on the prevalence and costs of tobacco use among Ugandan police officers is vital in adducing attention to tobacco use among this high-risk group and to undergird occupationally relevant policy and prevention interventions.
METHODS
This study was a cross-sectional survey conducted between August and October 2018 at Nsambya Police Barracks, Kampala City, Uganda. Participants were enrolled on a voluntary basis and informed consent was obtained. A total of 349 police officers were recruited to participate in the study. The primary aim of the study was to investigate prevalence of smoking, attitudes towards smoking, costs, and factors influencing cigarette smoking in the Ugandan Police Force. The effect of variables, such as education, gender, rank, occupational status, smoking by a close friend and deployment abroad, on smoking police officers were also investigated. ‘Police officer’ as used in this study implies law enforcement personnel of UPF and includes both gazetted and non-gazetted officers.
Survey methods
A 48-item tobacco questionnaire was employed based on one used by Basaza et al.1. The survey tool included sociodemographic, smoking breaks, quantity and frequency of smoking, sick days, attitudes towards smoking, and deployment history. All questionnaires were self-administered and participants were assured of confidentiality and anonymity of their responses. In order to test for content and reliability of the tool, we undertook a pilot study prior to the start of the main survey with 20 police officers representing 5% of the total sample size from the same barracks. Reponses from the pilot sample were not included in the data presented for the larger survey. Total costs of a smoker per year is the sum of lost productivity due to smoking breaks, and absenteeism and presenteeism costs attributable to cigarette use. This method was based on the human capital approach used to calculate lost productivity in statistical modeling by Berman et al.22.
Current smoker status meant smoking cigarettes every day or occasionally, in the last 30 days. Non-smoker status was defined as former and never smokers. Police officers eligible for inclusion in the study were those aged 18–54 years. Eighteen years represents the youngest acceptable age of recruitment in UPF that has mandatory retirement age of 60 years. However, the selected age range for inclusion was consistent with similar studies done in the military, facilitating comparisons among these two occupations1,23.
Sampling pattern covered study geographical setting and participants. We used a multistage cluster sampling strategy to construct the study sample. Purposive sampling was used to select Nsambya Police Barracks, the largest police barracks in Uganda located in Kampala City. The city was one of the earliest districts to implement policies designed to restrict tobacco use in public places and it has had a reputation for enforcement and compliance of the law, estimated at 72%24. Study participants were selected using stratified and systematic random sampling. Two strata were modeled to suit the purpose of the study, the SF (special support forces) and GGD (guard and general duties) units. The participants solicited were 20% from SF and 80% from GGD of the sample size, consistent with the total number of police officers in each category. Study sample target was 396 (i.e. 316 from GGD and 80 from SF). The homes in the units of the barracks counted in the cluster were numbered and only even numbers were visited to solicit respondents in the survey. The International Health Sciences University Faculty Research Committee provided ethical approval to conduct this study. The research team obtained signed consent from participants and no uniquely identifying data were included in the database.
Statistical modeling
Economic models were adopted from similar previously published studies1,22. Lost productivity attributable to tobacco use among police officers was calculated using the annual-cost approach (i.e. human-capital approach). Under this approach, cost of smoking per year was projected using cross-sectional data. We used cost analysis to assume that factors, apart from smoking, influenced both smokers and non-smokers equally22,25.
Data were analyzed using Epidata Version. 3.5.4 and Statistical Package for Social Science (SPSS) Version.16 for windows. Variables were loaded into Epidata V. 3.5.4 for descriptive statistics and frequency tables and then exported to SPSS V.16. Logistic regression analysis was used to model the association of sociodemographic indicators with smoking. The results are presented as odds ratios and their 95% confidence intervals. For each indicator the control group or most advantaged group was selected as the reference category. P-values <0.05 were considered to be statistically significant.
RESULTS
Prevalence and risk factors of smoking
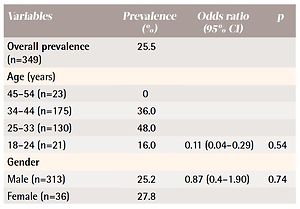
Among officers invited to participate (N=349), 88.1% completed and returned the questionnaire (Table 1). The highest number of respondents were in the age group 34–44 years (n=175, 50%), followed by 25–33years (n=130, 37%), 45–54 years (n=23, 7%), and 18–24 years (n=21, 6%). The mean age of participants was 27 years (SD=0.7) and the average length of service as a police officer was 2.42 years (SD=1.01). The highest prevalence of smoking was in the age group 25–33 years at 48.0 %, followed by 34–44 years at 36.0%, and 18–24 years at 16.0%. There was no smoker in our sample registered in the age group 45–54 years. Age was a non-significant factor affecting smoking (OR=0.11; 95% CI: 0.04–0.29; p=0.54). Among the officers, 25.2% of males and 27.8% of females reported being current smokers, rates which are markedly higher than the general Ugandan population (16% males vs 3% females). Risk factors for smoking included higher educational attainment, younger age, occupational status and having close friends who smoke.
Table 1
Prevalence of smoking stratified by demographics and risk factors (N=349)
| Variables | Prevalence (%) | Odds ratio (95% CI) | p |
|---|---|---|---|
| Overall prevalence (n=349) | 25.5 | ||
| Age (years) | |||
| 45–54 (n=23) | 0 | ||
| 34–44 (n=175) | 36.0 | ||
| 25–33 (n=130) | 48.0 | ||
| 18–24 (n=21) | 16.0 | 0.11 (0.04–0.29) | 0.54 |
| Gender | |||
| Male (n=313) | 25.2 | 0.87 (0.4–1.90) | 0.74 |
| Female (n=36) | 27.8 | ||
| Education | |||
| Primary (n=7) | 0 | ||
| Senior (n=243) | 18.1 | 3.76 (2.25–6.29) | <0.01 |
| College (n=99) | 45.5 | ||
| Rank | |||
| Constable (n=209) | 27.8 | 1.15 (0.34–3.90) | 0.81 |
| Non-Commissioned | 15.9 | 2.35 (0.63–8.81) | 0.20 |
| officer (n=82) | |||
| Junior officer (n=45) | 31.1 | 0.98 (0.25–3.74) | 0.98 |
| Senior officer (n=13) | 30.7 | ||
| Occupational status | |||
| Guard & General Duties | 29.9 | 1.08 (0.39–2.9) | 0.87 |
| (n=234) | |||
| Administration (n=65) | 20.0 | 1.84 (0.58–5.78) | 0.292 |
| Health Personnel (n=19) | 31.5 | ||
| Other (n=31) | 0 | ||
| Close friend smokes | |||
| Yes (n=71) | 39.4 | 2.31 (1.33–4.03) | 0.003 |
| No (n=278) | 21.9 | ||
| Deployment abroad* | |||
| Yes (n=62) | 33.9 | 1.64 (0.90–2.96) | 0.10 |
| No (n=287) | 23.7 |
Overall, 36.1% of the respondents reported that smoking is harmful to the health of both users and those who are exposed to tobacco smoke. Alarmingly, 62.9% of smokers and 64.5% of non-smokers did not consider smoking harmful to health. However, a large majority of participants (81.9%) believed smoking was a burden on the national economy. Despite the enacted law spelling out a punishment of imprisonment not exceeding more than seven years and/or a fine not less than UGX4.5 million for failing to comply with smoke-free ordinances, 59.6% of smokers and 49.2% of non-smokers agreed that Ugandan tobacco control laws are weak and ineffective.
When we analyzed the impact of serving in the police force, about 58.4% of participants initiated smoking and 67.4% smoked for the first time in the initial 6 months of their employment. A majority (59.6%) of police officers reported that the primary reason they smoked was to cope with stress, followed by peer pressure (14.6%). Respondents reported that their typical smoking pattern had not significantly changed since they started smoking.
Costs of smoking to the UPF
Absenteeism
Average days absent from work per year was much higher among smokers compared to non-smokers (23.2 versus 3.8 days). Given an average rate of UGX709 per hour and 9 hours per day work (the standard 8-hour work plus 1 hour of unpaid overtime), smoking costs UGX123795 per smoking police officer per year due to lost workdays.
Lost productivity
Based on the survey outcomes, an estimated average time for a smoking break was 10 minutes. Smokers reported consuming approximately 10 cigarettes per day. As in previous studies conducted in Uganda1, we conservatively assumed that half (i.e. 5) of the cigarettes were smoked during their duty day. All personnel are provided three sanctioned breaks per duty day. We assumed that smokers took an additional two non-sanctioned breaks per day to smoke, consistent with previous research1. Given these assumptions, personnel who smoke spend 32.56 minutes per day in additional work breaks. Police officers in Uganda work on average 234 days per year (i.e. calendar year less weekends and public holidays). Thus, excess breaks due to smoking costs UGX180063 per smoker per year (i.e. 2 breaks × (32.56/60) × UGX709 × 234 days). We conservatively excluded the costs of premature death given that it typically does not result in employer costs, particularly for the police where personnel are relatively young.
Presenteeism
Productivity and performance among smokers are lower at work due to nicotine addiction25,26. We conservatively assumed a 1% decrease in productivity due to presenteeism based on a similar study done in Uganda1. The lost productivity due to presenteeism was UGX14931 (1% × UGX709 per hour × 9 hours × 234 days) per smoker per year.
Excess health care costs to UPF
According to Berman et al.22, the excess health care costs due to smoking per smoking employee can be calculated as: employer healthcare expenditure × adjusted smoking attributable fraction (SAF)/number of smoking employees. The estimated healthcare costs per person in Uganda is US$591. There are approximately 44601 active duty police officers in the UPF. Thus, total healthcare costs are estimated as $59 × 44601 or about US$2.631 million. We found a current smoking rate of 25.5%. As in previous research, we assumed an 8% SAF in the calculation of excess healthcare costs. Thus, the excess costs of healthcare due to smoking is estimated as ($2631459 × 0.08)/11883=US$17.72 per smoker or US$210448 in total.
Overall costs of smoking to UPF
Lost productivity due to smoking (absenteeism + smoking breaks + presenteeism) costs the UPF UGX1.796 million per year per smoker or UGX20.43 billion in total (1796174 × 44601 × 0.255) for active duty personnel. This is approximately US$5.521 million. Adding the excess costs of healthcare due to smoking to this figure results in a total cost of smoking to the UPF of US$5.731 million.
DISCUSSION
The smoking rate among UPF was 25.5% compared to 5.3% of the general population. The relatively high smoking rate in the UPF places a substantial burden on a police force that is understaffed and a country with limited financial resources. Importantly, cigarette smoking poses a national security risk due to its negative impact on UPF personnel health and readiness. Further, the rate of smoking among UPF was similar to high rates found among police officers in other countries. For example, Khan et al.27 found a 25.4% current smoking rate among police in Bangladesh. Thus, there is a need for targeted tobacco interventions in this high-risk occupation. We recommend that the UPF: 1) design and implement organizational tobacco control policies to eliminate tobacco use at the workplace; 2) educate their officers about the negative impact of smoking on health and readiness; and 3) develop intervention programs designed to prevent and treat tobacco dependence among officers. Given that UPF officers may serve as role models to Ugandan youth and are tasked to enforce the national tobacco control laws, encouraging personnel to avoid tobacco should be a national public health priority.
As with our previous study of the Ugandan military, this study demonstrates that although the rate of smoking is relatively low in Uganda’s general population, certain occupations have relatively high rates of usage. This suggests that similar occupational groups, such as prison guards and firefighters, may also evidence high rates of tobacco use. Thus, additional studies are needed to provide an insight on the smoking situation in all first responder and uniformed occupations.
Limitations
There are some limitations to this study. First, the study was conducted only at the large police barracks of Nsambya in Uganda, and although the barracks is typical of the UPF, additional research is needed to ensure the results are generalizable to the police as a whole. There may be urban and rural differences in tobacco consumption. Some studies have found that smokers living in rural areas are more likely to smoke 15 or more cigarettes per day than smokers living in urban areas27. Second, the skip interval used to identify even-numbered homes assumes that odd-numbered homes were not significantly different. However, we saw no reason to suspect that the homes differed and using this skip-interval method reduced study burden. Third, self-reporting might have introduced some bias or led to under-reporting of true cigarette prevalence due to police officers’ regulatory obligations in law enforcement. However, this study found a relatively high rate of self-reported cigarette use despite the risk of under-reporting. Fourth, lost productivity associated with cigarette smoking contains instances where cigarette smoking may play a coincidental rather than a causal role. If so, the higher costs of healthcare might be associated with, rather than caused by, smoking. Fifth, police officers rotate between different duty stations in similar environments including outdoors. Thus, we could not easily ascertain the effect of outdoor environment of the smoking patterns. Last, no qualitative data were collected, which may have provided more insight into factors influencing cigarette smoking among police officers.
CONCLUSIONS
Tobacco use among the Ugandan Police Force represents a significant burden to a country’s health system that is struggling with poor infrastructure, limited health workers and infectious diseases. Importantly, cigarette smoking poses a national security risk due to its negative impact on police force readiness. Thus, there is an urgent need for tailored tobacco interventions and organizational policy for the Ugandan Police. Our recommendations and study findings are applicable in the context of the increased consumption rate in police officers compared to the general population, which we largely attribute to the nature of the profession. In addition, the police profession is male dominated and as such this study’s results may allow inferences for men in particular and the rest of the population in general.