
INTRODUCTION
Comprehensive smoke-free policy
The World Health Organization Framework Convention on Tobacco Control (WHO FCTC) is an evidence-based health and legally-binding treaty that requires its 181 Parties to implement evidence-based measures to reduce tobacco use and exposure to tobacco smoke1,2. Article 8 of the WHO FCTC refers to the need for protection from exposure to tobacco smoke3. It emphasizes the need for ‘100% smoke-free environments in all indoor public places, indoor workplaces, on all means of public transport, and, as appropriate, other public places’.
Workplace designated smoking area
Article 8 also stipulates that the use of designated smoking areas (DSAs) does not provide effective protection3. Nonetheless, DSAs still exist in public places in both developed and developing countries. Indoor areas for smoking are mostly common in airports and are considered as ‘smoking lounges’ while DSAs exist in many workplaces4. This situation is not in line with the WHO FCTC because Article 8 of the WHO FCTC highlights the need for a comprehensive smoking ban for effective protection from secondhand smoke. The FCTC does not recommend enclosed areas for smoking in public places or workplaces5.
It is interesting to appraise the qualitative study by Burton et al.6 who revealed that smokers never smoked in indoor designated areas but preferred to go outdoors to prevent others from being exposed to tobacco smoke6. Another qualitative study by Bondy and Bercovitz7 highlighted the need for a complete smoking ban on construction worksites, instead of making provisions for DSAs. On the other hand, Sherriff and Coleman8 revealed employers’ belief that they would violate the rights of their employees if they did not allow them to smoke on the worksite. It has also been reported by Kaufman et al.4 that community members considered law enforcement as a violation of smoker’s rights.
Workplace smoking cessation intervention
The evaluation of the first smoking cessation workplace intervention in Hong Kong showed that smoking cessation programs, chosen by smokers and supported by employers without further incentives, were feasible in a busy working environment9. A pilot clinical trial of smoking cessation services implemented in the workplace has demonstrated the feasibility and efficacy of providing workplace smoking cessation services10. A qualitative study exploring employees who were involved in a workplace smoking cessation programme showed that contributors to quit success were the workplace setting, quitting with colleagues, competition and motivation, as well as group strategies to resist smoking11. In Iowa, workplace smoking bans were nearly universal and two-thirds of the workplaces offered activities to help employees quit smoking within the context of the Iowa Smokefree Air Act; there was practically no barrier to adoption and implementation of workplace smoking cessation interventions12.
Controversy on human rights of smokers vs non-smokers
Graff13 confidently put forward the fact that ‘there is no constitutional right to smoke’. Referring to the 1948 Universal Declaration of Human Rights, Article 1 states that ‘All human beings are born free and equal in dignity and rights’14. Article 3 states that ‘Everyone has the right to life, liberty and security of person’14. Article 25 of the same Declaration mentions ‘health as part of the right to an adequate standard of living’14. Internationally, the right to health was first articulated in the 1946 Constitution of the World Health Organization15. The General Surgeon16 put forward that ‘Non-smokers have as much right to clean air and wholesome air as smokers must have their so-called right to smoke, which I would define as a right to pollute’. However, in the preamble of the WHO FCTC, the Parties expressed their determination ‘to give priority to their right to protect public health’3. Also, the preamble to the Constitution of the WHO states that ‘the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition’3.
Concerning Article 12 of the 1966 International Covenant on Economic, Social and Cultural Rights, ‘it is the right of everyone to the enjoyment of the highest attainable standard of physical and mental health’ (WHO 2003)3. Considering the Convention on the Elimination of All Forms of Discrimination against Women, adopted by the United Nations General Assembly on 18 December 1979, Parties will eliminate gender discrimination in the field of health care3. Focusing on the Rights of the Child, Parties to the Convention acknowledge ‘the right of the child to the enjoyment of the highest attainable standard of health’3.
In 2017, on the occasion of the Human Rights Day, health was emphasized by the WHO Director-General as a fundamental human right, with good health being the resultant of other basic human rights including access to safe drinking water and sanitation, nutritious foods, adequate housing, education and safe working conditions1. The WHO Director-General, in 2017, stated: ‘The right to health for all people means that everyone should have access to the health services they need, when and where they need them, without suffering financial hardship…’. The central principle of the 2030 Agenda for Sustainable Development is to ensure that no one is left behind.
Justification for the study
The Constitution of the Republic of Mauritius puts forward the protection of one’s right to live in a healthy environment as follows: ‘Everyone shall have the right to an environment that is not harmful to their health or well-being’17. Considering the no-smoking policy in public places in Mauritius, which has been implemented since 2008–09, smoking is banned in all indoor public places including indoor workplaces unless a DSA is available18. Therefore, the island of Mauritius does not have a comprehensive smoking ban in workplaces. The International Tobacco Control (ITC) team highly recommended the elimination of DSAs, emphasized as essential to protect non-smokers from exposure to tobacco smoke and to provide a smoke-free environment for smokers to quit19. The loopholes related to DSAs that exist in Mauritius, and certain legislations in other countries, prevent non-smokers to live in a 100% smoke-free environment.
This situation prevails because of the standpoint of trade unions in Mauritius. However, it is not in line with Article 8 of the FCTC3; it also does not align with Article 3 of the Universal Declaration of Human Rights that ‘Everyone has the right to life, liberty and security of person’14. At the local level, it is in contradiction with Chapter 2 of the Constitution of the Republic of Mauritius that highlights the protection of one’s right to live in a healthy environment as follows: ‘Everyone shall have the right to an environment that is not harmful to their health or well-being’17. DSAs in the workplace are controversial. Since the implementation of the non-comprehensive smoking ban in Mauritius, there has been no study to explore the views of stakeholders on this issue of DSAs in workplaces.
In light of the controversial status of the smoke-free policy in Mauritius, this study was designed with the following objectives: 1) to explore the perception of stakeholders on the DSAs prevailing in workplaces in Mauritius, and 2) to explore the feasibility of smoking cessation interventions in the workplace. It is the first research that puts forward the views of stakeholders on DSAs in workplaces in Mauritius. The outcome of this study is the provision of the means for policy makers in Mauritius, and other African countries, to address the gap in the implementation of comprehensive smoke-free policies.
METHODS
A qualitative approach was used to explore the views of representatives of the following stakeholders: Ministry of Labour, Ministry of Environment, Ministry of Health, Business Process Outsourcing companies (BPOs), Media, Trade Unions, Academia, and Non-Government Organizations (NGOs). Stakeholders were identified by a purposive sampling approach. Inclusion criteria were: adult, employed, literate, and consent. Participants were recruited until data saturation was reached. The number of interviewees was eight.
Conducted as per the Declaration of Helsinki, this study obtained ethical clearance from the Ethics Committee of the Department of Medicine of the University of Mauritius. Every participant was provided with a participant information sheet and consent form. All subjects provided informed consent before participation in the study. The semi-structured, face-to-face, individual interview was conducted in the participant’s office where privacy prevailed and the interviewee was comfortable and able to talk at ease. Data were collected using an audio recorder in addition to note taking. The duration for each interview was 20–30 minutes.
The interview guide comprised open-ended semi-structured questions. Collected data were transcribed verbatim. Thematic analysis, as discussed by Braun and Clarke20, was the method used for analyzing data collected and for identifying patterns within coded data, to generate themes. Each transcript was read several times to familiarize ourselves with the transcribed data. Important words or groups of words representing interesting features of the data were identified and highlighted as initial codes. Relevant codes were gathered to form potential themes. By reviewing the themes, the thematic map of the analysis was worked out. Fine-tuning to the naming of the themes was developed by the iterative ongoing process of analysis. Pertinent quotations from participants were selected in line with the research questions for the presentation in the report. Anonymity of participants was maintained during data analysis and presentation of findings.
RESULTS
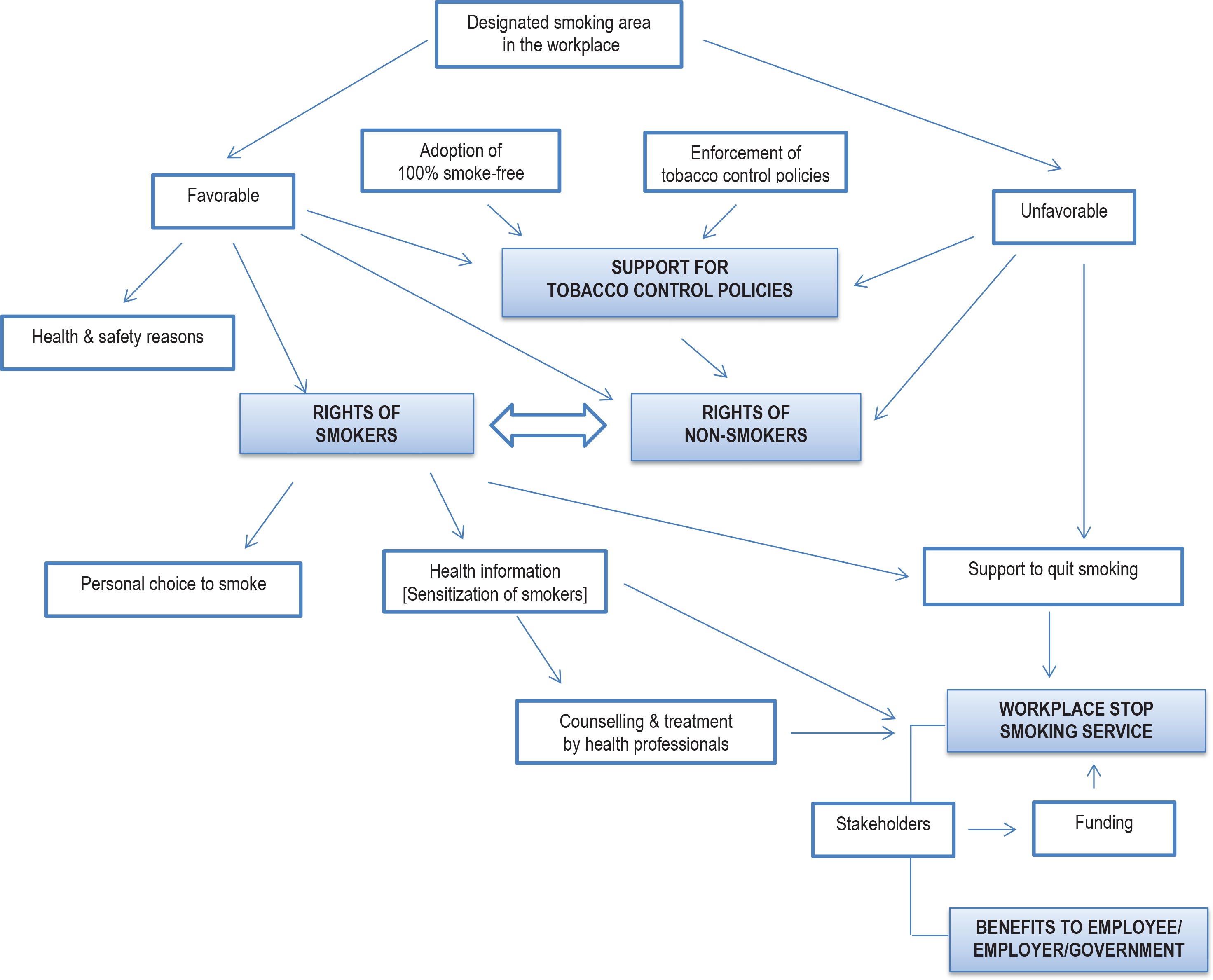
Data analysis led to the emergence of four main themes, with each main theme having two to four sub-themes, as shown in Table 1. Table 1 presents in a simplistic manner the themes generated. On the other hand, Figure 1 shows the findings of this qualitative study in a detailed manner.
Table 1
Main themes and sub-themes related to the perception of stakeholders
Figure 1
Generation of themes from the views of participants on designated smoking area in workplaces.
Theme 1: Support for tobacco control policies
The first theme has two sub-themes: strengthening the law by adopting a 100% smoke-free environment, and enforcement of the tobacco control policies.
Strengthening of the law by adopting 100% smoke-free environment
Regarding that Mauritius does not have a comprehensive smoking ban in workplaces, participants were in favour of strengthening the current tobacco control policies in Mauritius that allow workplace DSAs. Participants put forward the need to address the existing loophole about workplace DSAs to achieve a 100% smoking ban in workplaces. Stakeholders agreed that the WHO proposed an excellent initiative concerning the need for removal of smoking areas in all workplaces.
‘The elimination of tobacco smoke in all indoor workplaces including private offices is an excellent objective to be adopted by the WHO’. (1, M)
‘It [WHO’s recommendation] is a good objective taken by the WHO…’. (2, M)
‘I completely agree with the WHO and I think it is a good measure to eliminate smoking all public places and indoor workplaces…’. (3, M)
‘Being a non-smoker, I think that the WHO brought a very good idea which we [stakeholders] shall fully adopt in the future’. (4, M)
‘The WHO is right as the FCTC doesn't imply the existence of smoking areas’. (7, M)
‘I agree with the WHO for not recommending smoking areas on work premises. Their [WHO] aim is to help smokers to quit smoking’. (8, F)
Enforcement of current tobacco control policies
Participants shared the view that enforcement of current tobacco control policies should be addressed by implementing the existing penalties to non-compliant citizens.
‘Yes, indeed! Mauritius should implement stronger laws if they want to eliminate this silent killer across the island. Introducing more strict laws will also help to decrease the number of people diagnosed with lung cancer.’ (4, M)
‘Yes, Mauritius should reinforce the law for a healthier environment and increase security measures in terms of exposure to tobacco smoke’. (5, M)
‘I suggest that the government follows what the WHO had said and a further increase in tobacco taxation is required. We have already started to implement stronger laws…’ (2, M)
‘Mauritius needs to completely ban smoking in workplaces (…) If ever someone is caught smoking in non-smoking areas, we should fine them so that they will be discouraged to smoke’. (3, M)
‘…smoking areas are strictly prohibited in hospitals, educational institutions and in sports and recreational infrastructure. If these places have become smoke-free then we should extend the law into workplaces’. (6, F)
Theme 2: Actions for implementation of stop-smoking services
The second theme had four sub-themes: sensitization of smokers, identification of funding, provision of counseling/treatment, and involvement of stakeholders.
Sensitization of smokers
Participants shared the view that smokers should be provided with assistance to quit smoking. There is a need for smokers to have easy access to appropriate treatment to combat tobacco dependence. There is, thus, the need for sensitization campaigns among employees to inform them about tobacco-related diseases and to promote tobacco cessation. Sensitization needs to focus on the benefits of smoking cessation. However, effective sensitization programs should be convincing, motivating, and attractive, otherwise smokers would be reluctant to quit. There is a need for the stop-smoking services to be attractive and interactive.
‘Firstly, we should help them to stop this bad habit of smoking and educate them on lung cancer which is associated with smoking…’. (4, M)
‘We should give them information on how to stop smoking because that person needs help as he or she is addicted to nicotine’. (6, F)
‘A good initiative is to sensitize the smoker about the impact of cigarette on the health’. (8, F)
‘Instead of giving negative information, we should inform them about the benefits of smoking cessation and at that moment the person will realize its advantages’. (6, F)
Identification of funding
The workplace smoking cessation program was viewed in terms of resources such as finance, counselors, and the time availability of employees. The cost-effectiveness of smoking cessation programs was put forward.
‘…we need resources such as funds and manpower (…) it is not easy to implement such programs because there are too many resources which are unavailable. The medications are expensive …’. (7, M)
‘…there will be lots of work in terms of money to do health campaigns and volunteers to participate in this project’. (8, F)
Provision of counseling and treatment
In addition to educational support, smokers need to be provided with counseling and nicotine replacement therapy.
‘In addition to information about smoking cessation, we should provide them with psychological and pharmacological treatment. We should provide them with all the necessary treatments to help them quit’. (6, F)
‘I think that sensitization of all employees is essential and should provide them with alternatives for tobacco such as nicotine gums to prevent carvings’. (2, M)
Involvement of stakeholders
All respondents agreed that both the government and employers should be responsible for organizing tobacco cessation programs with the help of health professionals.
‘It would be amazing if the Ministry of Health could assign some health professionals or officers to inform these people…’. (1, M)
It was put forward that employers should be involved in providing these programs.
‘…actions should be taken from the Ministry of Health and the Civil Society. Health professionals especially doctors should be recruited to prescribe medical treatment and qualified counselors such as health educators are needed to provide support to these people’. (7, M)
‘… not only through the intervention of the Ministry of Health but the company may also hire private health professionals to help his employees to quit smoking’. (6, M)
‘Employers should also take action by introducing cessation programs and sensitize the employees (…) the employers may organize committee forums whereby employees will benefit advice from governmental organizations’. (3, M)
Participants underlined the importance of the company’s involvement in providing treatment for tobacco dependence.
Theme 3: Benefits of workplace stop smoking services
Further data analysis revealed the emergence of sub-themes related to the benefits to employees, company, and country. Improvement of the health of employees, the enhanced reputation of the company, and benefits to the economy of the country will be illustrated with the quotes of participants.
Benefits to employees
Benefits to employees ‘As these smokers quit smoking, they will save money and their health will start to improve …’. (6, F)
‘If we go towards these people, it would be very beneficial to them. They would be more available to attend the programs (….). The programs should be flexible so that employees will not be absent from work to follow this program’. (7, M)
Benefits to the company
‘… start providing these types of programs to their employees as it will lead to healthy people working in the company and increase in its productivity’. (4, M)
‘…the productivity of the company is increased and there will be a decrease in absenteeism due to tobacco-related diseases’. (6, F)
‘…the time taken for the program must not be greater than their time taken to smoke’. (2, M)
Theme 4: Controversy on the human rights of smokers and non-smokers
Last but not least, the human rights of both smokers and non-smokers were discussed. It was thought that a complete smoking ban and removal of DSAs will prevent smokers from being free. However, it was also acknowledged that smoking is harmful to non-smokers and violates their right to live in a 100% smoke-free environment.
DISCUSSION
We now discuss the four themes that emerged from this qualitative study in the following sub-sections: controversy on the human rights of citizens, need for smoking cessation services, benefits of workplace smoking cessation programs, and support for tobacco control policies. The outcome of the discussion leads us to put forward a solution to the issue of workplace DSAs.
Controversy on the human rights of citizens
In this study, participants perceived that smokers have a right to smoke, provided that they do not smoke in restricted areas. Participants who had expressed support for DSAs on work premises perceived that a comprehensive smoking ban will deprive smokers of their rights to freedom. This finding is in line with Sherriff and Coleman8 who revealed employers’ belief about employees’ rights to smoke on the worksite and also with Kaufman et al.4 who reported the perception of community members about smoker’s rights. However, these views do not corroborate with Article 3 of the Universal Declaration of Human Rights, which does not mention the ‘right to smoke’ (Graff13).
Participants in this study referred to the right of non-smokers to be free from exposure to tobacco smoke. This finding is in line with Katz21 who stated that failure to provide a smoke-free environment would transgress the individual’s right to lead a healthy life. The WHO put forward the role of public health law reform to advance the right to health and to create an environment for people to live healthy lives22. Smoking is rather a personal choice than a human right. The choice of a person to start smoking is his or hers. Nonetheless, the personal choice of a smoker impedes the rights of non-smokers for unpolluted air, in line with the well-known phrase ‘my liberty ends where yours begins’. Quote Investigator on its website23 states that the authoritative source of the origin of this quote has not been found but considers Finch (1882) as the one who stated: ‘Your right to swing your arm leaves off where my right not to have my nose struck begins’. From the same website23, we can read that Camp (1887) made the statement: ‘I have no right to throw my arms out in a crowd, for I might hit somebody on the nose. My right stops where his nose begins. I have no right to drink if my drinking injures others’. By extension, we will put forward: ‘I have no right to smoke if my smoking affects others’.
Need for smoking cessation services
One of the four major themes emerging from this qualitative study was: actions for the implementation of stop-smoking services. Referring to the contribution of stakeholders in tobacco cessation programs, participants pointed out the role of three pillars, namely the government, employers, and health professionals, in such programs. Health professionals need to be recruited by the Ministry of Health for workplace health promotion that includes smoking cessation services. The findings of this study are in line with the study among hospital staff in Egypt. Radwan et al.24 demonstrated the urgent need for the provision of smoking cessation programs to both medical and administrative staff of hospitals (85.4%) and the provision of smoking cessation training for physicians (84.8%). Another finding from this qualitative study pertains to the view that employers are to be involved in sensitization programs. This is also in line with Radwan et al.24 who highlighted the need for the establishment of a tobacco control committee in hospitals (81%) and the provision of logistical support for tobacco control programs and policies (77%).
Benefits of workplace smoking cessation programs
Benefits for the country, highlighted by participants, are in line with various studies demonstrating cost benefits. The very recent mathematical modeling by Honeycutt et al.25 showed that the potential costs of interventions were substantially larger than actual costs. Benefits included savings in terms of medical costs in the range US$700–750 million and in terms of life-years gained in the range of 21000 to 22000 years. More than a decade ago, Warner et al.26 had shown that smoking cessation was a significant economic investment for companies with long-term benefits with a benefit-cost ratio of nearly 9 times. Benefits for employees include financial savings and health improvement upon successful smoking cessation. Mache et al.27 showed that the intention to quit smoking significantly increased over time with employees participating in smoking cessation intervention. Participants put forward that decreased absenteeism and increased productivity as favorable outcomes for the company providing smoking cessation services. These views are supported by Halpern et al.28 who demonstrated that absenteeism was significantly higher among current smokers than former smokers, with a significant decline with years following smoking cessation. Productivity assessment by peers showed significantly higher values for former smokers than for current smokers.
Support for tobacco control policies
Participants of this study expressed support for the adoption of a 100% smoke-free workplace environment, which shows that they are in favour of the removal of workplace DSAs. This is in line with the Article 8 of the WHO FCTC3, the recommendation made by the ITC19 for the removal of DSAs in workplaces, and the recommendation by Bondy and Bercovitz7 for a complete smoking ban on construction worksites7. Concerning the support for the adoption of a 100% smoke-free workplace environment in Mauritius, there is a need for the clause that allows the current existence of workplace DSAs to be removed from the law. We trust that the removal of workplace DSAs needs to be undertaken in a planned phase-out manner with the provision of supportive measures for smoking cessation services in the workplace.
The idea of a planned phase-out of workplace DSAs with the provision of smoking cessation services now leads to a new concept: workplace ‘Designated Stop Smoking Areas’ (DSSAs). A DSSA in the workplace is an area designated by employers to provide stop-smoking support to employees who smoke, resulting from a workplace policy to gradually divert smokers away from a DSA to DSSA for smoking cessation. Therapeutic means will include motivational group therapy, dedicated individual counselling, and tobacco treatment prescription by tobacco treatment specialists to be made available in DSSAs. The right to have access to smoking cessation services when and where smokers need them, as specified by the Director-General of the WHO1, justify the new concept of DSSA. Also, the principle of leaving nobody behind lends support to the provision of support to smokers having difficulty to quit smoking.
Recommendations
This qualitative study led to a new concept: workplace DSSA, which will help to address the issue of DSAs in the workplace. We recommend the creation of DSSAs in the workplace in Mauritius while maintaining DSAs during a period of one or two years with planned phasing out of DSAs for comprehensive smoke-free workplaces in Mauritius. The role of three main stakeholders, the government, employers, and health professionals has been highlighted for the implementation of smoking cessation interventions in the workplace in Mauritius. Finally, this innovative call for DSSAs is meant to sensitize policy makers of developing countries on how to proceed for the elimination of DSA.
Strengths and limitations
This is the first qualitative study in Mauritius whereby the views of stakeholders were explored. However, the duration of interviews was limited in light of the busy schedule of the stakeholders. The number of participants was only eight, but it was verified that saturation of data was reached.
CONCLUSIONS
Data generated from this qualitative study led to the formulation of a new concept, the workplace DSSA, as a solution to the workplace DSA, which still prevails in some countries despite the WHO emphasis on the need for 100% smoke-free workplaces. This new concept provides policy makers the means to address the breach, constituted by DSA, in the implementation of comprehensive smoke-free policies. The new workplace DSSA concept provides the means for phasing out DSAs in developing countries where there are DSA-related loopholes in their legislation. The proposed workplace policy will also be useful to developed countries in their endeavour to achieve a comprehensive smoke-free environment.