
INTRODUCTION
Cigarette smoke is an intricate mixture of chemical substances that are attached to aerosols or are free in gaseous phase. Current research suggests that cigarette smoke includes more than 4000 chemical compounds1,2. Numerous classes of chemicals present in cigarette smoke are triggers for various diseases1-3.
The tobacco leaves are rich in alkaloids, but nicotine is the most abundant. Therefore, the alkaloid content includes: nicotine N'-oxide, myosmine, β-nicotyrine, cotinine, 2,3'-bipyridyl, anabasine, nornicotine, N-methylanabasine, anatabine, anabaseine and nicotine2,3.
Nicotine has numerous harmful effects and is well known to be very addictive. Nicotine is a dibasic substance and its absorption is related to the pH of the solution2. There are three forms of nicotine and all have great solubility in water and dissolve easily in blood2.
Therefore, nicotine has the ability to increase the quantity of free radicals and reactive oxygen species that trigger oxidative damage and cause tissue suffering. Also, nicotine stimulates the nuclear factor kappa B (NF-κB), which is implicated in inflammatory processes and cell damage2. Cigarette smoking damages nearly every organ of the body and induces the marked detrimental effects on the endothelial cells of the blood vessels. It causes increased endothelial cell proliferation and intimal hyperplasia. The vasoconstricting effects of smoking damage the oxygenation of the adjacent tissues4,5. Some of these negative effects are immediate while others are slower. Cigarette smoking causes oxidative stress with harmful effects on humans. Age-related macular degeneration (AMD) is a gradual degenerative impairment of the retina associated with damage of central vision6. The retinal pigment epithelium (RPE) contains a large quantity of melanin. RPE melanin plays a photoprotective role by absorbing radiation and contributing to the elimination of free radicals7,8. Melanin suffering and microvascular insufficiency are important causes in the pathogenic processes of AMD9-11. The cochlea is a structure of the inner ear which has in componence the organ of Corti and stria vascularis. Melanocytes are abundant in the inner ear and stria vascularis includes most of the melanin12,13. Melanin defends the structures of the inner ear against oxidative damage14-16. One side effect of cigarette smoking is decreased oxygen supply to the cochlea. This may result in constant hardship of the cochlea and moderate to severe hearing damage17. Also, cigarette smoking increases the risk of developing macular degeneration18. The correlation between simultaneous retinal and cochlear impairment may be due to melanin dysfunction and microvascular damage19. Melanin deficiency might initiate the apoptosis of retinal pigment epithelial cells and cochlear elements which are abundant in melanin. Oxidative stress caused by cigarette smoking triggers microvascular abnormalities and melanin deficiency, therefore smoking is highly associated with risks of hearing and visual loss16,20-22.
METHODS
In our analytic study, hearing and smoking status of 40 patients with AMD were compared with 40 agematched control subjects without AMD. All subjects were referred to the Ocularcare Eye Clinic during a 12-month period from March 2019 to March 2020. The study protocol was approved by the ethics committee of ‘Victor Babes’ University of Medicine and Pharmacy, Timisoara, Romania. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
The study population was represented by patients aged 65–75 years. In all individuals, retinal changes were validated by fundoscopy and optical coherence tomography (OCT), by analysis of thickness central subfield (TCS) and thickness average cube (TAC) of the macula. Cases and controls were excluded if they had other infectious inflammatory or retinovascular disorders, such as diabetic retinopathy, hypertensive retinopathy, retinal vascular occlusion or retinochoroiditis that could confuse the diagnosis of degenerative maculopathy. Based on Wisconsin age-related maculopathy grading system (WARMGS), the term AMD is attributed to geographic atrophy (GA), retinal drusen, choroidal neovascularization (CNV) and pigment epithelial detachment (PED)9. Patients were enrolled as cases if they had AMD in one or both eyes. Subjects without AMD were accepted in the control group.
Audiometry
All patients were inspected with pure tone audiometry. Audiometric trials comprised pure tone audiometry at frequencies ranging from 125–8000 Hz. Pure tones were used to analyze air and bone conduction. Audiometry was performed by using an AMPLIVOX LTD series 240 Portable Audiometer by an experienced audiologist. The cases of congenital hearing loss and the subjects who did not collaborate on audiometric trials were excluded from the study. The audiometric investigation was done to establish the type and the degree of the hearing impairment. The severity of the hearing loss was classified as normal (≤20 dB), mild (>25 dB and ≤40 dB), moderate (>40 dB and ≤60 dB), and severe (>60 dB), based on the pure tone average. The allotment into normal hearing, conductive, mixed and sensorineural hearing loss was done in conformity with the audiometric results.
Smoking history
Smoking data were assembled in the same way for both cases and controls. Smoking status was assessed as non-smoker and current smoker. The smoking group included patients that had a history of more than 10 cigarettes/day. Patients from the non-smoking group had no history of smoking. The questionnaire comprised the number of cigarettes smoked per day in each decade of life, exposure to passive smoking and use of other tobacco products. To acquire pack-years of smoking, the number of years of smoking was multiplied by the number of packs of cigarettes smoked per day2.
Statistical analysis
The statistical analysis was performed by using SPSS, version 22.0. Data assayed using logistic regression models for categorical variables are presented in relation to a reference category. The variables such as smoking status, type of hearing and vision damage, thickness central subfield and thickness average cube of the macula were reported as numeric variables. The results are summarized as odds ratios with 95% confidence interval (CI), with significance set at an alpha level of 5% (p≤0.05).
RESULTS
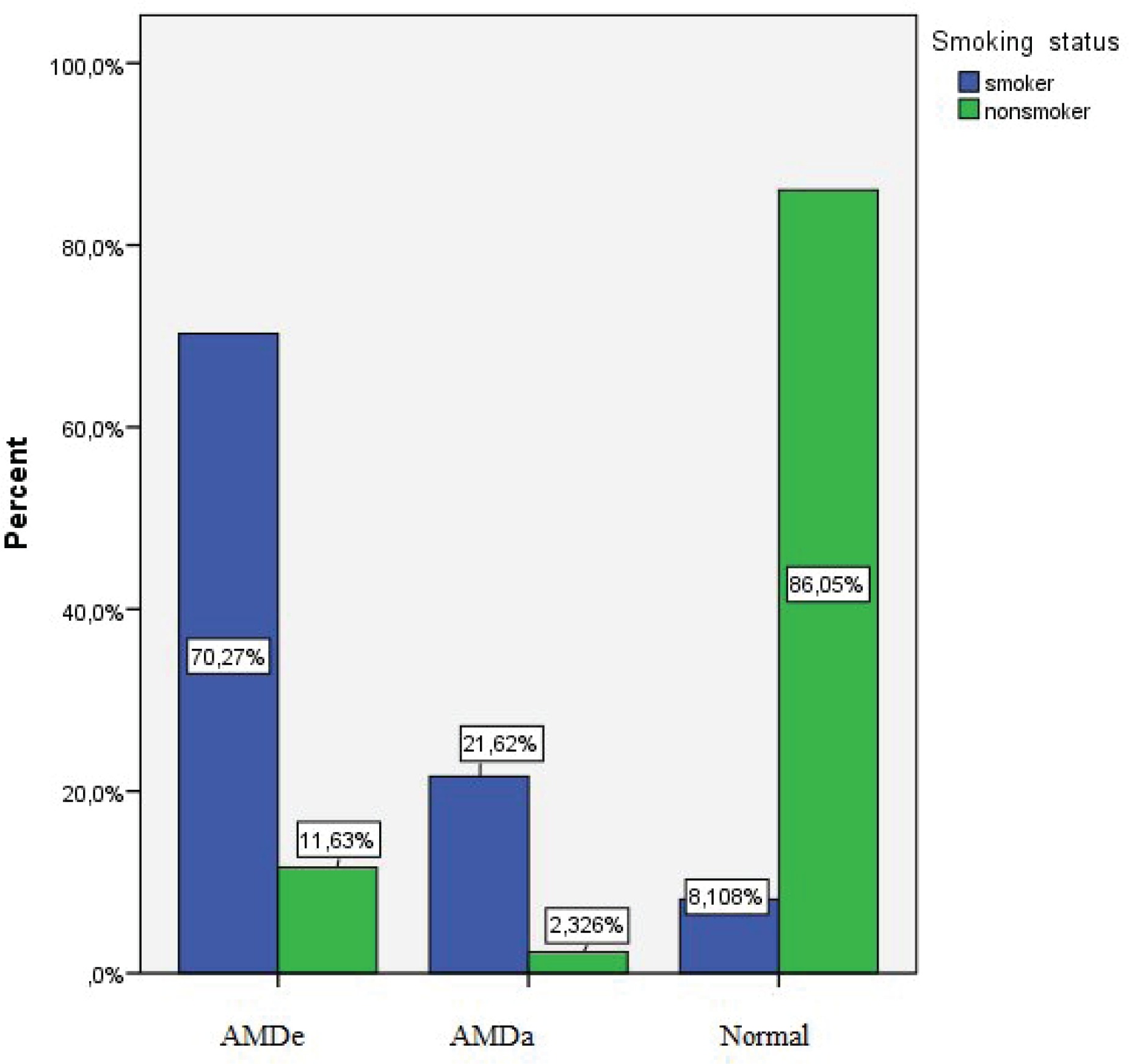
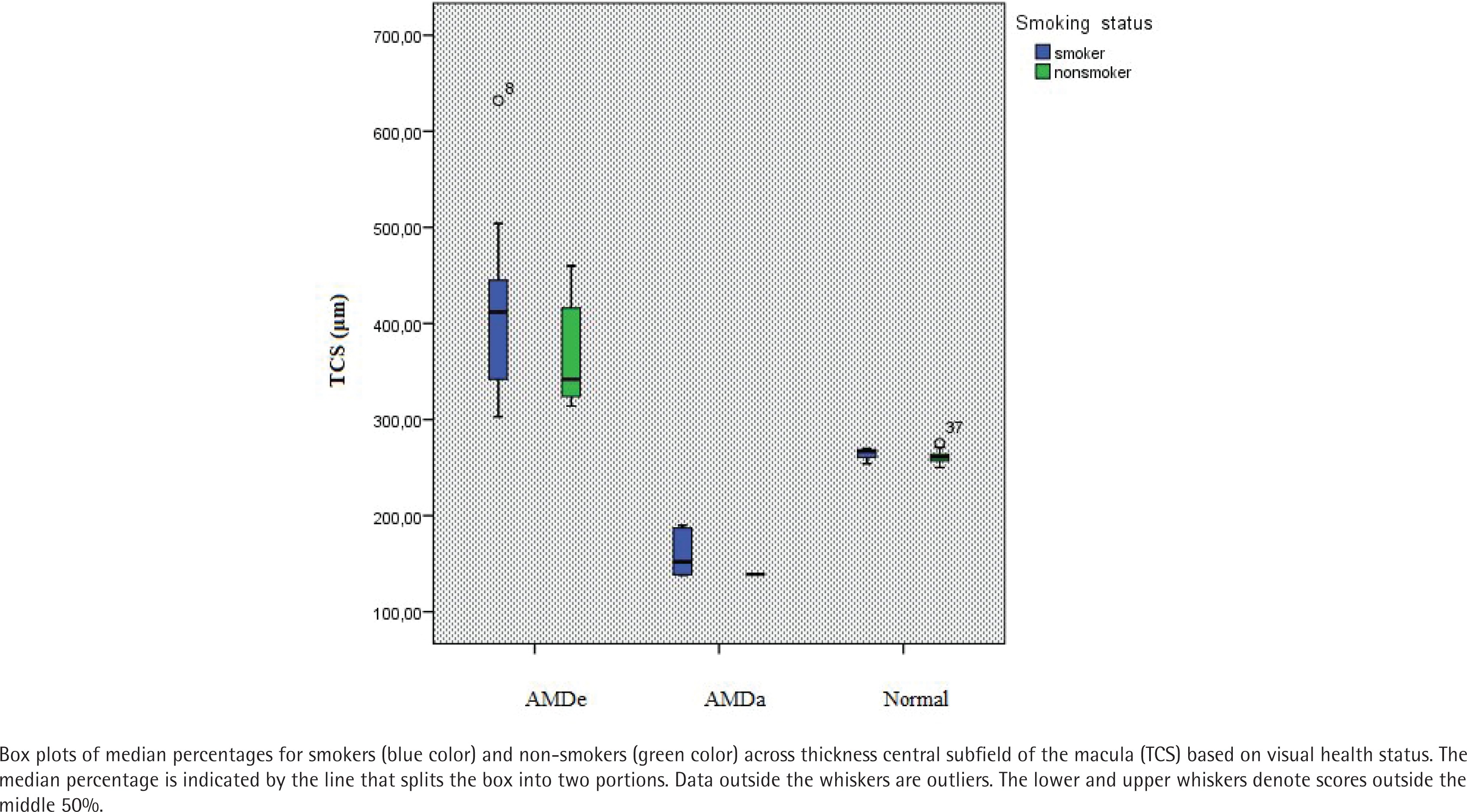
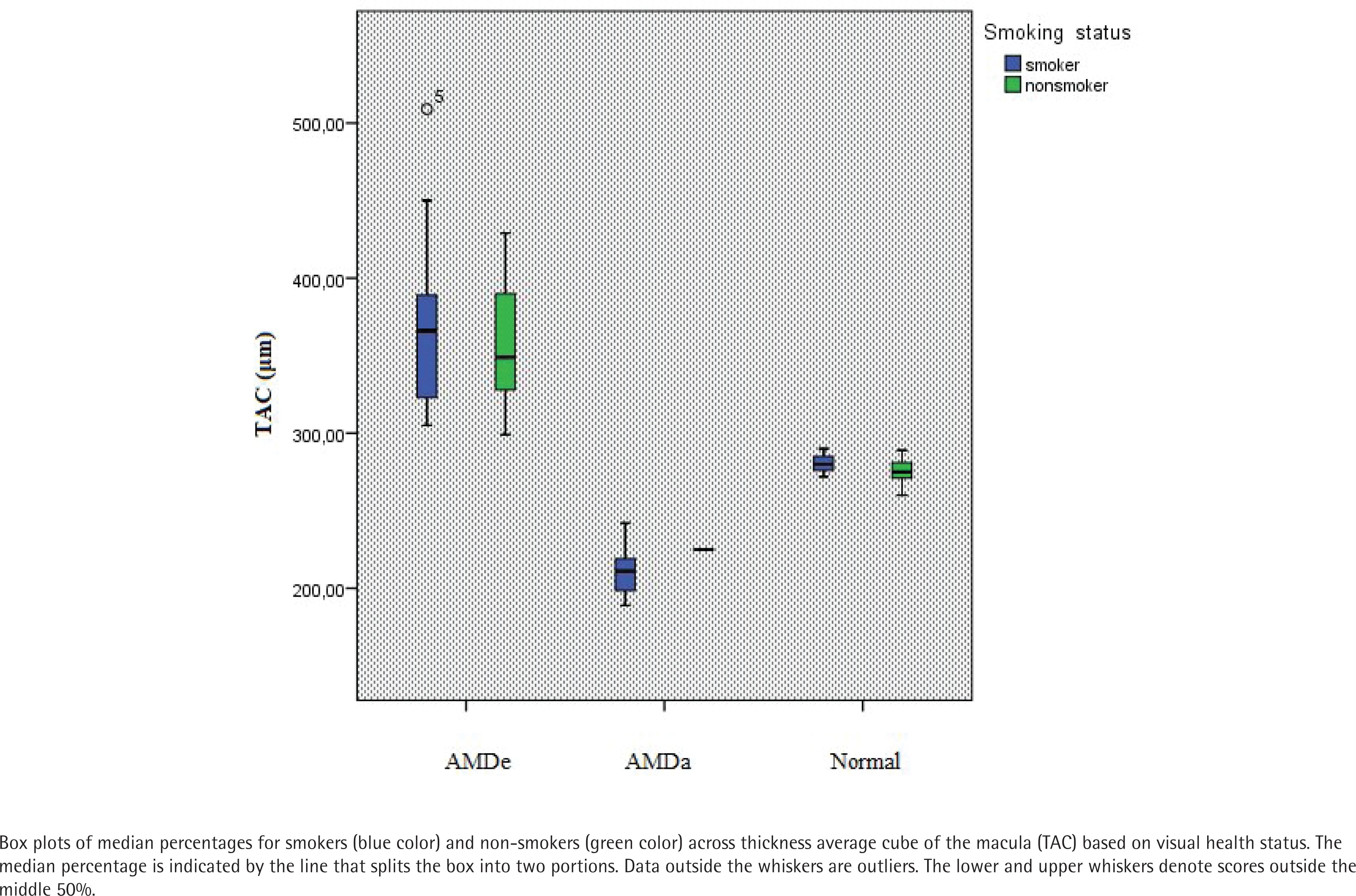
The study included 40 patients with AMD and 40 age-matched control subjects without AMD. Summary data and smoking history are presented in Table 1. The mean age of cases was 67.2 (SD=5.5) years and of controls was 68.4 (SD=4.2) years. On analyzing the audiometric results, it was noticed that cigarette smoking was found to be statistically associated with hearing impairment (p<0.05) (Table 2), especially sensorineural hearing impairment (HN), thus 75.68% of smokers were identified with sensorineural hearing loss (Figure 1). No statistically significant difference was found among other types of hearing loss. Regarding the correlation between age related macular degenaration (AMD) and smoking status, we noticed that 70.27% of smokers had exudative macular degeneration (AMDe) and 21.62% had atrophic macular degeneration (AMDa) (Figure 2), respectively (p<0.001) (Table 2). No significant consequence of cigarette smoking on thickness average cube (TAC) was detected (Figure 4). However, smoking affected the foveal thickness (TCS) (Figure 3).
Table 1
Age, sex and smoking data for cases and controls
Table 2
Hearing and visual health conditions according to smoking status
Figure 1
The effect of smoking on hearing status (N–normal hearing, HN– sensorineural hearing loss, HT–conductive hearing loss, HM–mixed hearing loss)
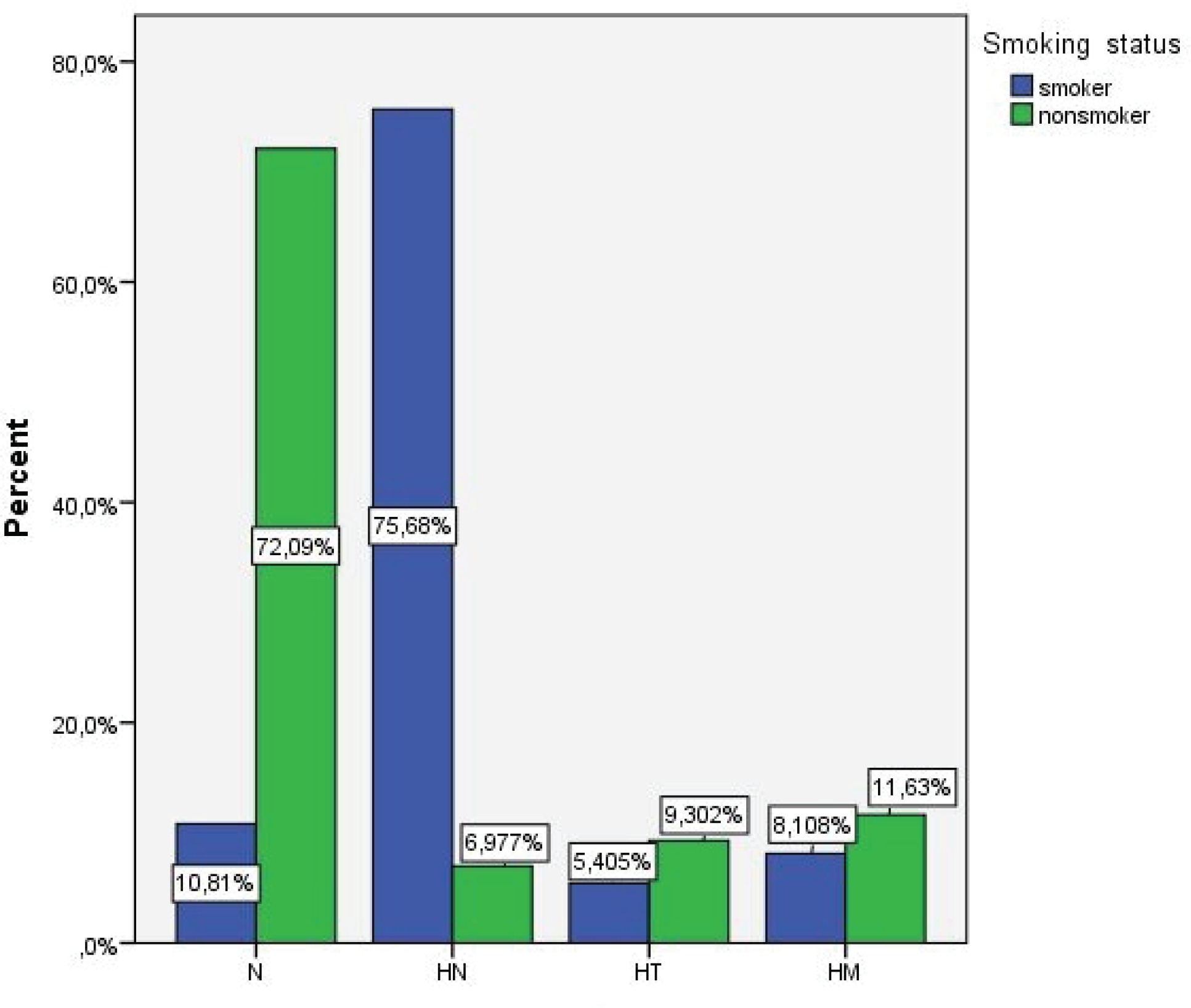
Figure 2
Relationship of cigarette smoking and visual impairment (AMDa–atrophic macular degeneration, AMDe–exudative macular degeneration)
DISCUSSION
In the current study, cigarette smoking was found to be statistically correlated with sensorineural hearing impairment. Sensorineural hearing impairment (HN) is caused by distress of the cochlear sensory epithelium or the peripheral auditory neurons. The sensory component is due to damage of organ of Corti or to an insufficiency of hair cells to stimulate the auditory nerve. The neural element refers to when damage is proximal to the cochlea and auditory nerve (retrocochlear damage)23-25. Conductive hearing loss (HT) is characterized by obstruction or illness in the outer or middle ear. Consequently, a mixed hearing loss (HM) implies a combination of conductive and sensorineural hearing damage, respectively the problem occurs in the outer or middle and the inner ear25,26.
Several distinctions were noticed in terms of smoking status between AMD patients and control group. Conventionally, AMD has been classified into two main categories: exudative (AMDe) and nonexudative or atrophic (AMDa). AMD is a common cause of irreversible central vision loss. Patients with AMD in one eye have about a 50% probability of developing AMD in the contralateral eye27-30. The complete diagnosis is based on fundoscopy and optical coherence tomography (OCT) which can differentiate exudative and atrophic types of macular degeneration. Optical coherence tomography (OCT) allows us to analyze in vivo the retinal layers. Macular thickness parameters such as thickness central subfield (TCS) and thickness average cube (TAC) are very important for analyzing retinal changes and to distinguish normal macular features from atrophic or exudative changes30.
The present study revealed that cigarette smoking shows a significant association with visual and hearing impairment. Consistent with our study findings, other studies have reported a highly significant association between current smoking and sensorineural hearing loss and age-related macular degeneration4,17,18,28. Cigarette smoking has pernicious effects on the retinal tissues and inner ear. This provides powerful support for a causal relation between cigarette smoking and the prevalence of sensorineural hearing loss and age-related macular degeneration.
Two phases have been recognized in cigarette smoke, gas and tar phases, which are abundant in free radicals and non-radical oxidants. Particularly, hydroxyl radical and peroxyl are implied in oxidative stress and tissue malady. We emphasized the hint of possible similar roles of melanin in progress of these two disorders in the retinal tissues and inner ear. Stria vascularis in the Corti structure of the cochlea is the basic structure including melanocytes. The number of Corti structures and melanocytes is lower at the base of the cochlea. Small melanin concentration makes the cochlear base more responsive to oxidative stress and lipofuscin aggregation. One way through which the chemicals found in cigarette smoke may produce an effect on hearing status, is by provoking injury to the anti-oxidative systems and to the ear vasculature2,28. On the other hand, melanin in the RPE cells defends photoreceptors against oxidative stress29. Melanin dysfunction as the most important fact in AMD, determines low to severe visual loss and blindness. In fact, RPE cells and photoreceptors act as a functional unit for the visual system30. Therefore, melanin alteration caused by oxidative stress might account for important concomitant visual and hearing impairment31-33. Cigarette smoke is known to be rich in chemical compounds5. The two most toxic constituents of cigarette smoke are nicotine and carbon monoxide, however, cigarette smoke contains about 4000 additional toxic components. Cigarette smoking decreases the blood supply due to the vasospasms induced, favors the atherosclerotic narrowing of the blood vessels and accelerates ischemic damage due to increased blood viscosity and by thrombotic occlusions with endothelial changes of the vessels34,35. One of the means through which the chemicals found in cigarette smoke may have an effect on cochlea is by causing vasculopathy. Besides this, chemicals found in cigarette smoke damage cochlear melanin. Also, the oxidative stress and microvascular damages provoke deficiencies in the metabolic bed of RPE with apoptosis of photoreceptor cells. Cigarette smoke implies a great number of prooxidant compounds4,36 and also consists of dioxins, which are moderated by aryl hydrocarbon receptor (AhR), which is a ligand-dependent transcriptional factor widely expressed among immune, epithelial, endothelial and stromal cells in barrier tissues. Dioxin affects ocular tissues through the AhR pathway, develops vascular endothelial growth factor (VEGF) production in human RPE cells which potentiates retinal exudation by neovascularization37-39.
Strengths and limitations
Due to a group of subjects who did not collaborate on audiometric trials, we had to exclude them from the study. Despite these limitations, important information were obtained. Baseline data regarding the nocive influence of cigarette smoking on the retina and the inner ear can be used to establish future cessation and prevention strategies.
CONCLUSIONS
We outlined the hypothesis of possible similar roles of melanin and microvascular abnormalities in development of retinal degeneration and hearing impairment. We also would like to emphasize the role of cigarette smoking on these disturbances. It seems to have two mechanisms. One is provoking injury to the anti-oxidative systems, the other is inducing vasculopathy and damage to tissue metabolism.