
INTRODUCTION
Tobacco smoking is the largest preventable health risk in the European Union (EU), contributing to 0.7 million deaths annually1. Smokers die on average 10 years younger than non-smokers from vascular, neoplastic and respiratory diseases, but this risk is halved if abstinence is achieved before the age of 50 years, and is almost completely avoidable with cessation before the age of 30 years2.
It is estimated that in an average year, around one-third of current smokers will make an attempt to quit3. Amongst those who make an attempt, only a minority are still abstinent a year later, with studies reporting abstinence rates at one year of 6–20%3-5. Research indicates that most relapses occur in the first six months following a quit attempt and these are associated with biological, social and psychological factors6.
Recent literature suggests that there are two elements in smoking cessation: the decision to make an attempt and maintaining abstinence. Studies have found that those of higher socioeconomic status, with lower levels of nicotine dependence and greater self-motivation to quit are more likely to make a cessation attempt7,8. With regard to successful cessation, while some studies have found associations between individual factors including gender, age and education attainment with successful cessation9-11, others have found mixed and inconsistent evidence between sociodemographic factors and successful cessation12. However, there seems to be more consistency in evidence suggesting that higher socioeconomic status (SES) is associated with increased likelihood of cessation9,13. Additionally, studies looking into sociodemographic factors associated with quit attempts are typically country-specific and most have been performed in individual countries, which may not translate directly to an EU-wide context14,15. Therefore, much uncertainty remains around sociodemographic as well as country-level predictors of a successful quit attempt.
Furthermore, there is mixed evidence surrounding the role of e-cigarettes in smoking cessation. A cross-sectional study across 28 European Member States showed that amongst current and ex-smokers who ever tried to quit smoking, 10.6% attempted using e-cigarettes, and amongst those who tried to quit in the past 12 months, 43.6% tried to do so with e-cigarettes, suggesting rising popularity of e-cigarettes as a cessation method16. While some studies, such as one amongst English former and current smokers performed by Brown et al.17, suggest a higher abstinence rate when using e-cigarettes as a cessation method, others, including a systematic review by Kalkhoran and Glantz18, have found no or a negative association between e-cigarette use and successful cessation16,18,19. Further clarification of the role of e-cigarettes in cessation could have important public health implications due to their rising popularity and general belief that they are less harmful than tobacco smoking20,21.
In addition, there is much variability in the definition of successful cessation, from abstinence at 6 weeks, 3 months, to one year14,15,22,23. Considering the variability of interventions and the different types of smoking cessation aids used in cessation research, it is difficult to standardize and compare results across studies. Studies estimating population-level smoking cessation also often employ the ‘quit ratio’, which measures the number of former smokers as a proportion of ever smokers (current plus former smokers)9. While this allows results to be comparable across cohorts and between countries, again it offers limited information on the temporality of smoking cessation, which could be helpful in assessing the impact of tobacco control policies, for example.
To supplement the current evidence, we conducted an analysis of the 2017 wave of the Eurobarometer survey in order to evaluate current progress in smoking cessation and explore potential predictors of recent successful smoking cessation across 28 EU Member States. This allows us to compare data and examine factors associated with successful cessation across 28 different countries and on a European level, and to potentially explore how national and EU-wide policies might be associated with smoking cessation as well as identify countries or population groups that may need additional support.
METHODS
Data source
The main data were obtained from the Special Eurobarometer 87.1 (March 2017) conducted by the European Commission across 28 EU Member States (MS) between 18 and 27 March 201724. A multistage probability sampling strategy was used to identify representative samples of the population aged ≥15 years. Primary sampling units (PSUs) proportional to population size were selected from regions of each country, and households were selected systematically through a standard random route. The household member whose birthday was closest to the date of the interview was selected. Face-to-face interviews were conducted in participants’ own homes in an appropriate national language. Resultant self-reported data were weighted for age, sex and area of residence for analysis. The total sample size was n=27901. The full methodology and questionnaire are published in the Eurobarometer summary report1. No ethical approval was required as the data sets are publicly available, and no identifiable data were used. The data underlying the results presented in the study are available from the Eurostat data base, available from https://ec.europa.eu/eurostat/web/main and also the European Commission Eurobarometer 87.1 2017:ZA6861 doi:10.4232/1.1292 available from https://dbk.gesis.org/dbksearch/sdesc2.asp?no=6861&db=e&doi=10.4232/1.12915.
Measures
Smoking status
Participants’ smoking status was assessed with the question: ‘Regarding smoking cigarettes, cigars, cigarillos or a pipe, which of the following applies to you?’. Those who answered ‘currently smoke’ were classified as ‘current smokers’ and those who answered ‘used to smoke but have stopped’ were classified as ‘former smokers’.
E-cigarette use
Use of electronic cigarettes was assessed with the question: ‘Which of the following statements about the use of electronic cigarettes or any similar electronic devices (e-shisha, e-pipe) applies to you?’. Those who responded ‘currently use electronic cigarettes or similar electronic devices (e.g. e-shisha, e-pipe)’ were classified as ‘current e-cigarette users’.
Smoking cessation attempts
We identified a subset of current and former smokers who made a recent quit attempt, approximately within the last 12 months before the date of the survey. Past attempts to quit in current smokers were assessed using the questions: ‘Have you ever tried to quit smoking?’ with the answers providing a time frame (‘Yes, in the last 12 months’, ‘Yes, more than a year ago’ and ‘No, never’). Those who answered ‘Yes, in the last 12 months’ were included in our analysis as ‘unsuccessful quitters’.
Former smokers were not asked the same question in the survey. We therefore combined two variables, current age and the age at which the respondent reported to have stopped smoking. Those who quit at an age 0 to 1 year younger than their current age were considered to have quit smoking approximately within the last 12 months, although it has to be noted that, based on this definition, this group could potentially include respondents who quit smoking up to 24 months before the survey. We classified them in our analysis as ‘recent quitters’ and we refer to their last quit attempt as ‘successful’, although this does not necessary imply long-term cessation.
To estimate likelihood of abstinence following a recent cessation attempt on a population-level, we introduced and estimated the new concept of ‘Cessation Ratio’, which we defined as the ratio of the number of recent quitters to unsuccessful quitters, as described above, for each of the 28 EU MS (Cessation Ratio = recent quitters/unsuccessful quitters). Based on this definition the Cessation Ratio could take any value ≥0. For example, a value of zero means that none of the smokers who recently attempted to quit was abstinent at the time of the survey; a value of one means that half of those who recently attempted to quit (recent quitters + unsuccessful quitters) were abstinent at the time of the survey; values higher than one imply that a majority of those who recently attempted to quit remained abstinent at the time of the survey. This is different to the commonly used ‘quit ratio’ which estimates the proportion of former smokers amongst ever smokers (current and former smokers).
Socioeconomic data
The survey also collected self-reported demographic data including age (15–24; 25–39; 40–54; ≥55 years), gender (male; female), age leaving formal education (≤15; 16–19; ≥20 years), area of residence (rural; small town; large town), and European region of residence (Northern; Eastern; Southern; and Western Europe). Socioeconomic status was assessed with self-reported social class (higher class; upper middle class; middle class; lower middle class; working class) and a proxy measure for financial difficulty using the question: ‘During the last twelve months, would you say you had difficulties paying your bills at the end of the month?’. Those who answered ‘almost never/never’ were classified as not having financial difficulties and those who answered ‘from time to time/most of the time’ were classified as having some financial difficulties.
Country-level data
Prevalence of cigarette and e-cigarette use was estimated for each EU Member State using the relevant questions in the Eurobarometer survey. Data on the comprehensiveness and implementation of tobacco control policies were obtained from the 2016 Tobacco Control Scale (TCS)25. Each country is awarded up to 100 points for tobacco taxation (30), public and workplace smoking bans (22), public information campaigns (15), comprehensive advertising bans (13), effective health warnings on tobacco products (10), and smoking cessation treatment provisions (10). In this analysis, we have used the score for cessation treatment only (range: 4–9 points). The Gross Domestic Product (GDP) per capita and unemployment rates for each country in 2016 were obtained from the Eurostat database26.
Statistical analysis
Descriptive results are presented as weighted percentage with 95% confidence interval (CI). Regression results are presented as adjusted odds ratio (AOR) with 95% CI. The regression analysis was performed in a subgroup of the main data set, which included only respondents who attempted to quit smoking approximately in the last 12 months [n=1472, sum of recent (n=454) and unsuccessful quitters (n=1018) as defined above]. Weights provided by the Eurobarometer were applied to the subset analysis of this study and included in any statistical models employed; more details on weights are provided in the Eurobarometer summary report24. We used the Akaike Information Criterion to determine the optimal specification of the regression model. We explored whether a multilevel logistic regression model with EU Member States as a higher level of analysis would be more appropriate than a simple logistic regression model by conducting a Likelihood Ratio test, but it did not improve the fit of the model and hence we opted for simple logistic regression.
Our logistic regression model assessed the association between the odds of a successful quit attempt and age, sex, financial difficulties, the country’s TCS treatment score, and prevalence of tobacco smoking. We also assessed other sociodemographic factors including age of leaving formal education, area of residence, European region of residence and self-reported social class, as well as the other country-level factors described above. None of these improved the overall fit of the model or significantly associated with the outcome and therefore were excluded from the final analysis. After comparing multiple models with the inclusion of different variables using Akaike Information Criterion, including both linear and quadratic variations of smoking prevalence, we found that the quadratic form of the association between smoking prevalence and the odds of successful quit attempt was the one that fitted best with the data. As a result, our final logistic regression model assessing the odds of a successful quit attempt included age, sex, financial difficulties, TCS treatment score and prevalence of tobacco smoking (both linear and quadratic terms) as variables. We also conducted a sensitivity analysis with the full TCS score instead of the cessation-specific TCS score. In addition, we plotted unadjusted Cessation Ratios against smoking prevalence and present this in the Supplementary file.
All analyses were performed with Stata (version SE 15.1); the map was also created with Stata. Weights provided in the official Eurobarometer data set were used in all descriptive analyses to account for the sampling methodology. Observations with missing values were excluded from the analysis.
RESULTS
A total of 27901 participants were surveyed in March 2017, across 28 European Union Member States. Sociodemographic characteristics of survey respondents are summarized in Supplementary Table S1. Country-specific characteristics including GDP per capita, unemployment rate and TCS treatment scores are listed in Supplementary Table S2.
The prevalence of smoking across the EU was 26.1% (95% CI: 25.3–27.0) with large differences between countries, ranging from 7.2% in Sweden to 36.6% in Greece (Table 1). Similarly, there were large variations in prevalence of current e-cigarette use, ranging from 0.18% in Italy to 5.04% in the United Kingdom. Among current smokers, 14.9% (n=1018) had tried to quit in the last 12 months (unsuccessful quitters), while among former smokers, 8.8% (n=454) reported having quit up to approximately one year before the time of the survey (recent quitters). A total of 1472 respondents were therefore included in our analysis as having attempted to quit smoking in approximately the last 12 months; 61 observations (4%) were excluded due to missing values.
Table 1
Smoking and e-cigarette prevalence, and cessation ratios across 28 European Union Member States, Eurobarometer 2017 (N=27901)
| Country | Sample size | Smoking prevalence | Prevalence of e-cigarette use | Sample size included in cessation ratio analysis | Cessation ratioa (95% CI) |
|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | ||||
| Austria | 1001 | 28.3 (25.2–31.6) | 2.70 (1.74–4.15) | 28 | 0.645 (0.468–0.851) |
| Belgium | 1023 | 19.2 (16.6–22.0) | 3.52 (2.44–5.06) | 70 | 0.826 (0.410–1.240) |
| Bulgaria | 1044 | 36.0 (33.1–39.1) | 0.21 (0.05–0.84) | 23 | 0.214 (0–0.449) |
| Croatia | 1048 | 35.2 (32.2–38.3) | 0.36 (0.13–0.97) | 47 | 0.509 (0.186–0.833) |
| Cyprus | 501 | 27.5 (23.4–32.1) | 2.72 (1.46–5.01) | 35 | 0.578 (0.157–1.00) |
| Czech Republic | 1058 | 28.9 (26.1–31.9) | 1.27 (0.71–2.24) | 37 | 0.509 (0.143–0.875) |
| Denmark | 1000 | 18.6 (16.1–21.4) | 2.15 (1.36–3.38) | 68 | 0.653 (0.290–1.020) |
| Estonia | 1017 | 23.3 (20.4–26.5) | 1.50 (0.71–2.24) | 62 | 0.182 (0.045–0.319) |
| Finland | 1012 | 20.1 (17.5–23.0) | 1.27 (0.67–2.41) | 73 | 0.453 (0.214–0.692) |
| France | 1004 | 35.9 (32.6–39.4) | 4.43 (3.22–6.07) | 82 | 0.424 (0.209–0.639) |
| Germany | 1537 | 25.4 (22.9–28.1) | 1.80 (1.12–2.88) | 81 | 0.349 (0.129–0.570) |
| Greece | 1010 | 36.6 (33.5–39.8) | 2.66 (1.74–4.05) | 60 | 0.417 (0.172–0.662) |
| Hungary | 1053 | 26.6 (23.8–29.6) | 0.58 (0.23–1.47) | 32 | 0.588 (0.130–1.050) |
| Ireland | 1021 | 19.4 (16.9–22.2) | 2.01 (1.27–3.15) | 69 | 0.365 (0.162–0.568) |
| Italy | 1022 | 24.6 (22.0–27.5) | 0.18 (0.04-0.71) | 10 | 0.380 (0–0.912) |
| Latvia | 1004 | 32.2 (28.4–36.3) | 0.89 (0.36-2.20) | 105 | 0.481 (0.216–0.747) |
| Lithuania | 1001 | 29.1 (25.9–32.4) | 0.76 (0.28–2.10) | 58 | 0.516 (0.206–0.826) |
| Luxembourg | 510 | 21.0 (17.3–25.2) | 1.61 (0.71–3.64) | 31 | 0.347 (0.055–0.640) |
| Malta | 500 | 24.0 (19.7–28.9) | 1.95 (0.89–4.20) | 29 | 0.249 (0.015–0.482) |
| Netherlands | 1015 | 19.5 (16.9–22.2) | 1.67 (1.04–2.68) | 87 | 0.428 (0.217–0.639) |
| Poland | 1008 | 29.7 (26.7–32.8) | 1.10 (0.55–2.18) | 54 | 0.433 (0.163–0.702) |
| Portugal | 1061 | 25.6 (23.0–28.4) | 0.94 (0.48–1.80) | 25 | 0.632 (0.120–1.140) |
| Romania | 1033 | 28.0 (25.2–30.9) | 0.46 (0.18–1.15) | 32 | 0.292 (0.041–0.543) |
| Slovakia | 1014 | 26.3 (23.4–29.5) | 0.26 (0.08–0.85) | 40 | 0.301 (0.101–0.621) |
| Slovenia | 1027 | 27.9 (25.0–31.0) | 0.62 (0.22–1.71) | 36 | 0.399 (0.091–0.708) |
| Spain | 1024 | 27.5 (24.7–30.4) | 0.52 (0.21–1.25) | 59 | 0.434 (0.186–0.682) |
| Sweden | 1007 | 7.2 (5.3-9.7) | 0.30 (0.08–1.04) | 48 | 1.060 (0.262–1.860) |
| United Kingdom | 1346 | 17.4 (15.1–20.0) | 5.04 (3.75–6.75) | 91 | 0.594 (0.271–0.917) |
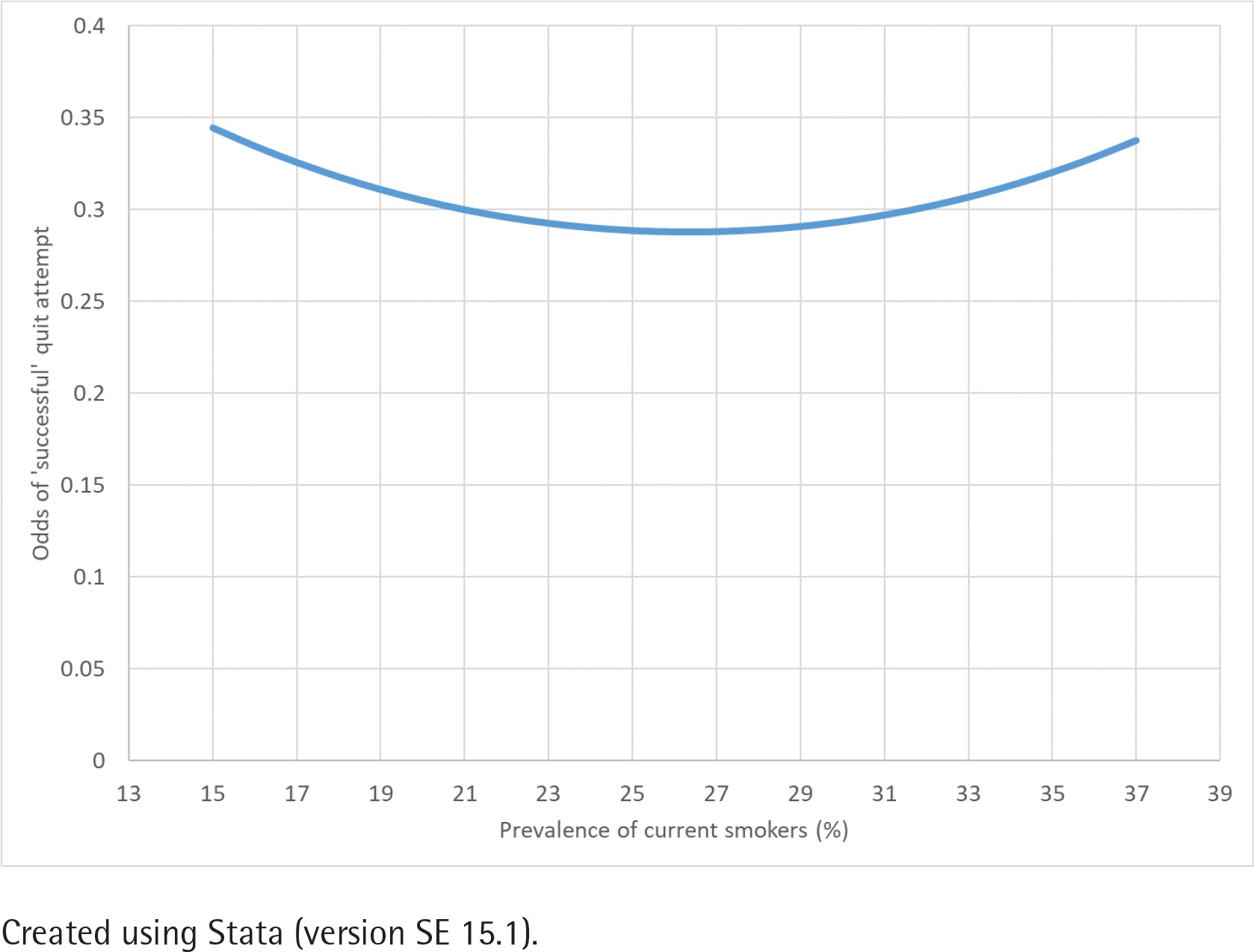
In our study subset, those with financial difficulties were less likely to have been successful in quitting than those without (AOR=0.66; 95% CI: 0.52–0.83; p=0.001) (Table 2). Gender, age, and TCS treatment score of the respondent’s country of residence had no significant association with successful smoking cessation. We found a significant quadratic, U-shaped relationship between the odds of having been successful in a recent quit attempt and smoking prevalence of the EU MS (Figure 1). After adjusting for age, sex and TCS treatment score, our model estimated that an individual had the lowest odds of having been successful in quitting when living in a country where smoking prevalence was 26.3%, with odds of success higher at each end of the prevalence spectrum. The sensitivity analysis conducted using the full TCS score instead of the cessation-specific TCS score yielded no significant difference to the main analysis.
Table 2
Associations of successful smoking cessation in past 12 months in 28 EU MS, Eurobarometer 2017 (N=1472)
Figure 1
Correlation between odds of success in quit attempt and smoking prevalence, Eurobarometer 2017 with extrapolation
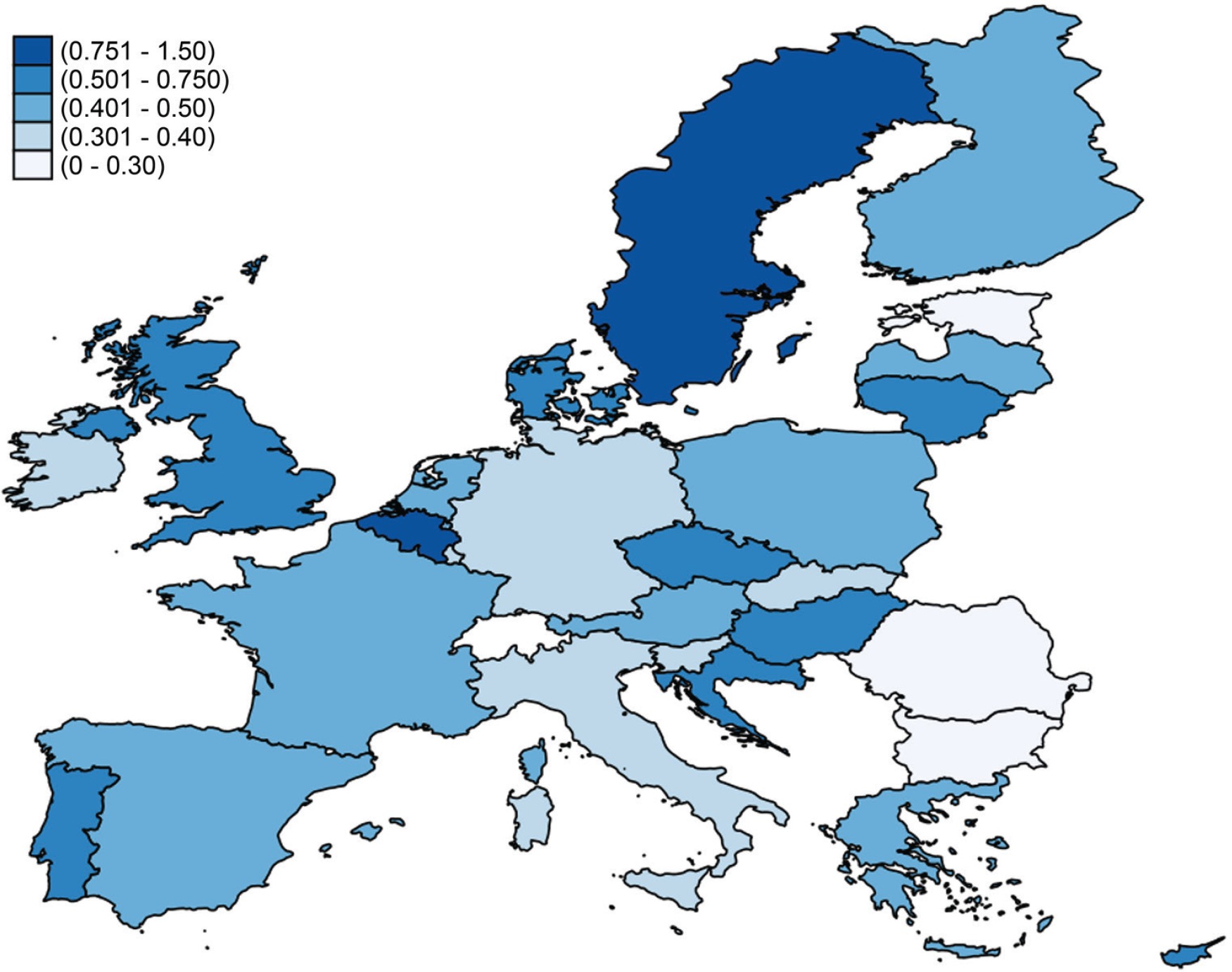
There was wide variation amongst EU MS in their Cessation Ratios, ranging from 0.182 (95% CI: 0.045–0.319) in Estonia to 1.060 (95% CI: 0.262– 1.860) in Sweden (Table 1 and Supplementary Figure S1). Only Sweden and Belgium had a Cessation Ratio above 0.7, indicating high success in smoking cessation, with the majority of MS (21 out of 28) between 0.3 and 0.6 (Figure 2). The choropleth map of Figure 2 was created using Stata (version SE 15.1) and republished from StataCorp under a CC BY license, with permission from StataCorp.
DISCUSSION
There is wide variation in the Cessation Ratios among the 28 EU MS sampled, with the highest Cessation Ratios found in Northern Europe. Amongst the study subset and on an individual level, having some financial difficulty, a proxy measure for SES status, was associated with a less successful quit attempt. We did not find significant associations between other sociodemographic factors including age and gender and the likelihood of a successful quit attempt. On a country level, we found a quadratic relationship between smoking prevalence and odds of a successful quit attempt. There were no significant associations between odds of success and a country’s GDP per capita, unemployment rate, prevalence of e-cigarettes or TCS treatment score.
In our analysis, some Northern European countries had higher Cessation Ratios compared to Southern European countries, although during our modelling no significant association between odds of success and European region of residence was demonstrated. Previous literature has suggested that Southern Europeans are less likely to use smoking cessation aids when attempting to quit27, which has been associated with lower likelihood of success, but this association is inconsistent28,29. Southern European countries may also have less comprehensive community healthcare and primary care framework to support smoking cessation activities, which can affect motivation, efficacy and likelihood of success30.
We found a quadratic relationship between the odds of quitting and smoking prevalence among our study sample, with a transition point at a prevalence of around 26.3%. The relationship was U-shaped indicating that the odds of quitting were optimal when smoking prevalence is either very low or very high. Although country-specific factors, such as socioeconomic and cultural differences between European countries as well as accuracy of self-reporting pose challenges in formulating an overarching explanation of this finding, it might reflect a true phenomenon. In communities where smoking prevalence is high, there may be a large number of smokers who are able to quit relatively easily when effective tobacco control measures such as smoking bans or tax increases are implemented. With lower – but still high – smoking prevalence, the proportion of ‘easy quitters’ might be lower, hence, smokers find it on average more difficult to quit. This could explain the upper end of the association and provide some support to the so-called ‘Hardening Hypothesis’31, although there has been a growing body of evidence against this where ‘hardening’ has not been demonstrated32,33.
However, on the other end of the U-shape relationship, the odds of success are higher where prevalence is lower. It is possible that when prevalence of tobacco smoking becomes quite low, smoking becomes denormalized and less socially appropriate, which might motivate smokers to quit and make them more effective in their quit attempts. This is echoed in existing literature32,33. There is also literature suggesting ‘softening’ of the smoking population as opposed to ‘hardening’ – with lower overall smoking prevalence, there could be a higher prevalence of ‘light smokers’ and a lower prevalence of ‘hardcore smokers’, and as a result the overall population-level likelihood of successful cessation increases34,35. Lower smoking prevalence also implies that there are more former smokers, who can provide support and serve as role models. This is supported by a study by Giovino et al.36 showing that self-efficacy for quitting, intention to quit and successful abstinence at ≥3 months are all higher where prevalence is lower. Self-efficacy itself is a predictor of successful cessation7,15, which could explain the trend we found.
We have also compared our findings, adjusted for individual factors of age, sex and TCS treatment score, against a plot between unadjusted Cessation Ratios against prevalence (Supplementary Table S3 and Figure S1). In the unadjusted plot, there appears to be an inverse association between Cessation Ratio and prevalence, but it is influenced by outliers (Sweden) and can be confounded by age and other sociodemographic factors which differ between EU member states, as they may be at different stages of the tobacco epidemic37. Once these individual factors had been adjusted, as in our analysis, the relationship becomes U-shaped and more complex, as demonstrated by our findings. Further research on this association may provide more clarity and disentangle the influence of individual and country-level factors.
We found a significant association between having financial difficulties, a proxy for socioeconomic status, and the odds of a successful quit attempt, which is in line with current evidence3,12,14,16,22,23. It possibly reflects the fact that having financial difficulties is likely a confluence of conditions that influence successful cessation, rather than an independent factor. Existing tobacco control policies have been found to be most effective in higher SES groups9, and having access to healthcare and therefore medical advice and cessation assistance through insurance, which are associated with higher likelihood of successful cessation5. In addition, lower odds of success have been demonstrated in high levels of nicotine dependence7,38, poorer mental health39,40 and living in a home that permitted smoking5, all of which are conditions that are more likely amongst smokers in lower SES groups41. These factors would be an important area for future research assessing associations with successful cessation, but have not been included in our study as they were beyond the scope of our data set.
Aside from socioeconomic status, we found no significant associations between other sociodemographic factors and odds of successful cessation. Earlier analyses have found similar results12,15,16. Although in one study males were found to be more likely to make a quit attempt10, they were not more likely to be successful.
Previous studies have shown that a higher TCS treatment score, or having policies to increase access to cessation aids, was associated with higher rates of smoking cessation42-44. In contrast, we did not find any association between TCS treatment score and having been successful in a recent quit attempt. However, our analysis was restricted to those who had made an attempt in the past 12 months. Treatment provisions could influence both a smoker’s decision to make a quit attempt and their chances of success through complex mechanisms; our study was not able to disentangle such associations but further research in this area would be beneficial to clarify the mechanisms through which availability of cessation support affects cessation efforts and success. For instance, there has been a significant increase in the use of e-cigarettes by the public as a smoking cessation aid45, but their effectiveness is still unclear and therefore have not been included in most national treatment efforts16-18,46. Our analysis echoes previous studies and did not find any significant positive associations between the prevalence of e-cigarettes and the likelihood of successful cessation16,18.
Strengths and limitations
The Eurobarometer survey is representative of the EU population aged ≥15 years and the sampling methodology has been standardized across 28 EU MS, allowing valid comparisons and generalization of results across EU populations. Although there can be discrepancies between the Eurobarometer and national surveys due to differences in phrasing, sampling methods and sample sizes, existing literature finds a positive and significant correlation between Eurobarometer and national survey data47. Our study also looks at attempts to quit within approximately the last 12 months, providing a more focused time frame and allows interpretation alongside any concurrent tobacco control policies. It improves upon the more commonly used quit ratio, which is a cumulative measure including all former smokers, regardless of when they achieved abstinence.
However, the selection of current and former smokers who were included in the analysis was based on different questions suggesting a slightly different time frame for recent successful or unsuccessful quit attempts. As a result, the Cessation Ratio we estimated should not be interpreted as an actual ratio of successful over unsuccessful quitters, which was impossible to estimate with the available data. Nevertheless, the standardized methodology of Eurobarometer across Member States allowed us to make country-level comparisons using this ratio as a proxy indicator of smoking cessation success. The sample of current and former smokers with recent quit attempts was small across the countries, which introduces uncertainty in some of the estimates. Additionally, although there is high agreement between self-reported cigarette use and biochemical testing48,49, self-reporting is less accurate for smoking cessation50,51, especially considering that Eurobarometer questions did not define a time frame for smoking abstinence.
CONCLUSIONS
Lower socioeconomic status was significantly associated with lower odds of a successful quit attempt, which could exacerbate existing health inequalities in the EU. We also found large variations in Cessation Ratios across the EU Member States. Future research could therefore explore any country-specific and individual factors that explain such differences, in order to inform policies that target specific populations. Finally, we reported a U-shape association between the odds of successful smoking cessation in the past year and smoking prevalence. Despite the limitations of our dataset, our finding suggests that there may be a critical threshold in smoking prevalence below which quitting becomes easier for remaining smokers who attempt to quit. This would be of great importance for nations which are aiming to reduce the burden of smoking.