
INTRODUCTION
The epidemic of disease caused by smoking ranks among the greatest public health catastrophes of the last century1-3. Despite this knowledge, smoking is still the leading preventable cause of death in the Western world1. In Denmark, the smoking prevalence has steadily decreased over many decades but has stagnated for seven years on a daily smoking rate of 17%4. Furthermore, the smoking prevalence among the young adults has increased in 2017, which is alarming4.
The health consequences of smoking have led to a range of public health initiatives. High cigarette taxes, smoke-free legislation, comprehensive marketing bans, media campaigns, smoking cessation treatment/clinics, and graphic health warnings have important roles in reducing the smoking prevalence5. A large body of evidence of the benefits of tobacco control exist, but the potential unintended consequences of this public health strategy have received little attention. Smokers report perceiving smoke-free legislation as increasing the stigmatization of smoking6. The social pressure placed on smokers might potentially lead to an increasing level of stress and social isolation, a feeling of increased resistance to quitting smoking and to increased relapse7. A recent experimental study showed that stigmatization led smokers toward emotional, cognitive, and attitudinal reactions that might make them less likely to quit smoking8.
Smokers in the general population have been found to have higher stress hormone levels than non-smokers9. Prospective studies have shown that a high stress level is associated with nearly double the odds of failure to quit smoking10 and experimental studies have shown that following a stressful event, smokers experienced increased tobacco craving, smoked more intensely and were less able to resist smoking11.
Large repeated cross-sectional surveys in the Capital Region of Denmark give us a unique opportunity to investigate the association between smoking and stress, at population level. To our knowledge, no previous studies have investigated the temporal changes in stress in smokers and non-smokers, at population level.
We hypothesized that, if tobacco control policies have increased the stigmatization of smokers, we would see a greater increase in stress in smokers than in non-smokers.
The aim was to investigate if Danish smokers in the general population reported high stress levels more frequently than non-smokers, if there has been an increase during the period 2010–2017 in citizens’ perceived high stress, and if the proportion of persons with high stress levels has increased more in smokers than in non-smokers. Finally, we wanted to describe the association between tobacco consumption and high stress level in daily smokers.
METHODS
The Capital Region, consisting of 29 municipalities, is the largest region of Denmark, with approximately 1.5 million inhabitants aged ≥16 years. Data were obtained (on paper or online) from repeated cross-sectional surveys of The Capital Region Health Survey conducted in 2010, 2013 and 2017. Random samples of all citizens were drawn from the Civil Registration System using computer-generated random numbers. Due to differences in population size among municipalities, one municipality increased the sample size to 4500 individuals, and Copenhagen Municipality was divided into ten areas, which were treated as individual municipalities in the sampling process. Each municipality drew a random sample of at least 2450 individuals (≥16 years). In 2017, the sample was increased to 4900 in four municipalities. Two to four reminders were sent.
The first survey, conducted in 2010, included a total sample of 95150 invited individuals. The final sample consisted of 49806 individuals (52.3% response rate). The second survey, conducted in 2013, included a total sample of 95150 invited individuals. The final sample consisted of 41356 individuals (43.5% response rate). The third survey, conducted in 2017, comprised a sample of 104950 invited individuals. The final sample consisted of 55185 individuals (52.6% response rate).
All citizens in Denmark are given a unique and permanent personal identification number at birth or on immigration, which allowed us to link data to national register data at the individual level.
The project was approved by the Danish Data Protection Agency. Approval from the Danish Health Research Ethics Committee System was not required according to Danish law. Written informed consent for publication of data was obtained.
Variables
Stress (self-reported)
Cohens Perceived Stress Scale (PSS-10) score was used12. PSS-10 consists of 10 items regarding predictability, controllability and life-overload, as perceived by the respondents during the past four weeks (range: 0–40). The higher the score, the greater the feeling of psychological stress. The scale has been validated and the Danish consensus version of the PSS-10 has good psychometric properties13. The PSS-10 was dichotomized into high stress level (PSS-10 ≥18) corresponding to the 20% with the highest score among respondents in 2010 and medium/low stress level (PSS-10 <18).
Smoking status (self-reported)
Smoking status was classified as: daily smoker, occasional smoker (‘yes, minimum once a week’ or ‘yes, less often than every week’), ex-smoker, and never smoker.
Tobacco consumption (self-reported)
Tobacco consumption was classified as: one cigarette/ gram of pipe tobacco = 1 g, one cheroot = 3 g, and one cigar = 5 g of tobacco.
Alcohol consumption (self-reported)
This was ascertained by the following questions: ‘Have you been drinking alcohol the last 12 months?’ and ‘How much alcohol have you typically been drinking every day during the week?’. The respondents were dichotomized into ‘as recommended’ (0–14 units per week for women and 0–21 units per week for men) and ‘above recommendation’, based on the recommendations of the Danish Health Authorities.
Loneliness (self-reported)
A Danish version of the Three-Item Loneliness Scale14 was used based on the following questions: ‘How often do you feel that you lack companionship?’; ‘How often do you feel left out?’; and ‘How often do you feel isolated from others?’. Response was evaluated on a 3-point Likert scale (hardly ever=1, sometimes=2, often=3). Higher scores indicate greater degrees of loneliness. Subsequently, the respondents were dichotomized into ‘being lonely’ (total score=7–9) or ‘not lonely’ (total score <7). The scale is based on the UCLA Loneliness Scale15, the gold standard measure in loneliness research.
Sociodemographic characteristics
Age, gender, educational level, cohabitation status and employment status were obtained from national registers at Statistics Denmark. Education and employment were used as indicators of socioeconomic position. The educational level was categorized into four groups based on the individuals’ highest level of completed education: ‘Basic/student’ (primary or secondary school only/under education); ‘Low education’ (up to two years of vocational training, e.g. carpenter, hairdresser); ‘Medium education’ (two to four years of education e.g. teacher, nurse); and ‘High education’ (four years or more of academic education, e.g. doctor, psychologist).
Employment data were obtained from the Income Statistics Register. Employment status was categorized as: ‘Employed/under education’; ‘Unemployed’ (unemployed, long-term ill, on disability pension); or ‘Retired’.
Statistical analysis
All analyses were weighted for survey design and non-response (higher among men, persons who were younger, had a lower income, were living alone, were unemployed, or/and were of an ethnicity other than Danish). The survey weights were computed by Statistics Denmark based on registry information about sex, age, municipality of residence, highest completed education level, income, civil status and hospitalization, for all individuals invited to the survey.
Descriptive results are shown as number of respondents and weighted percentage. Logistic regression analyses were used to investigate whether there were changes from 2010 to 2017 in self-reported high stress level, adjusting for sex, age, education level, employment and alcohol intake, and whether these changes differed with sex and across smoking status.
Logistic regression was used to investigate the associations between smoking status and high stress level using data from 2017, since information about loneliness was only available in 2017. The analyses were adjusted first for sex and age and then further adjusted for education level, employment, alcohol consumption, and loneliness.
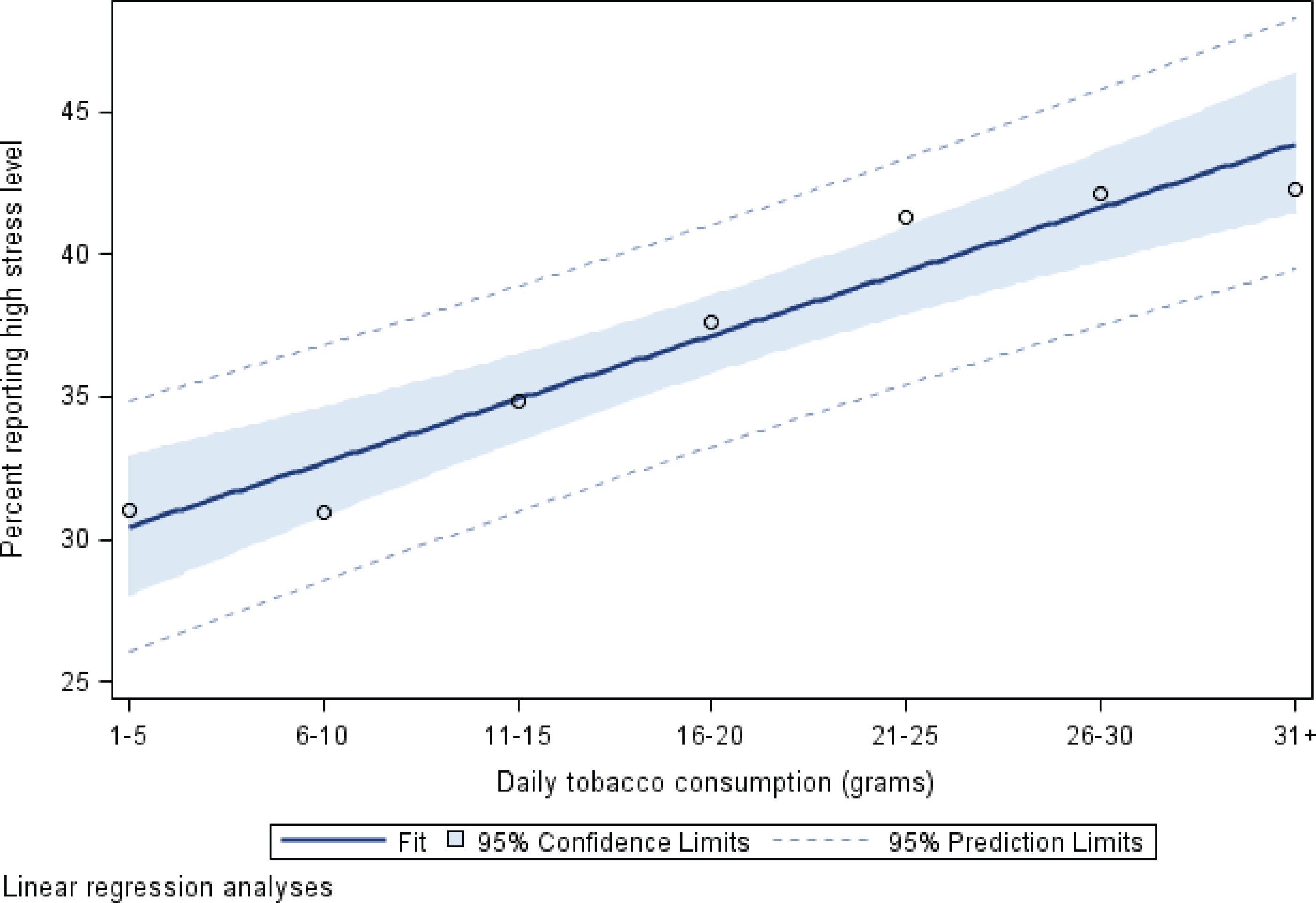
Nine categories for tobacco consumption (1–5, 6–10, 11–15, 16–20, 21–25, 26–30, 31–35, 36–40, ≥40 g) were created among daily smokers in 2017. The percentage of persons with high stress level was calculated within each of these categories. A linear regression was used to estimate the linear trend between tobacco consumption and high stress level. Statistical analyses were performed using SAS statistical software (version 9.4, SAS Institute Inc., Cary, NC, US).
RESULTS
The total number of respondents was 146347. Of these, 136608 reported both smoking status and PSS-10 and were included in this study. Characteristics of the population are given in Table 1, where approximately half of the respondents were aged 35– 64 years, there were slightly more women, and four in ten had a medium or high education. Three in four were employed and six in ten lived with a partner. In 2010, the median perceived stress score (PSS-10) was 11.4 (IQR: 7.0–16.3) and 22.1% reported a high stress level. In 2013, the median score was 10.5 (IQR: 5.9–15.8) and 20.6% reported a high stress level. In 2017, the median score was 11.5 (IQR: 6.5–17.1) and 25.5% reported a high stress level, and 16% were daily smokers (1% point lower than the national smoking rate). Daily smoking had decreased while occasional smoking increased over the seven years.
Table 1
Characteristics of the study population in Capital Region of Denmark in 2010, 2013 and 2017. Only persons with information on smoking and stress are included
| Characteristics | 2010 | 2013 | 2017 | |||
|---|---|---|---|---|---|---|
| n* | %** | n* | %** | n* | %** | |
| Sex | ||||||
| Female | 25909 | 51.3 | 21228 | 51.4 | 28679 | 51.2 |
| Male | 20391 | 48.7 | 16671 | 48.6 | 23730 | 48.8 |
| Age (years) | ||||||
| 16–34 | 10767 | 31.8 | 8204 | 32.4 | 11801 | 33.2 |
| 35–64 | 25601 | 50.7 | 19538 | 49.1 | 26731 | 47.2 |
| ≥65 | 9932 | 17.5 | 10157 | 18.6 | 13877 | 19.6 |
| Education level | ||||||
| Basic/student | 13836 | 35.0 | 10545 | 33.9 | 14295 | 34.0 |
| Low | 14239 | 28.2 | 11221 | 26.4 | 15343 | 25.0 |
| Medium | 11313 | 23.4 | 9814 | 24.5 | 13650 | 24.3 |
| High | 6059 | 13.4 | 5695 | 15.3 | 8377 | 16.7 |
| Employment | ||||||
| Employed/under education | 32431 | 73.0 | 25310 | 72.4 | 35815 | 72.7 |
| Unemployed | 2632 | 7.8 | 2107 | 8.0 | 3081 | 8.4 |
| Retired | 10235 | 19.2 | 9842 | 19.6 | 12088 | 18.8 |
| Cohabitation (age ≥25 years) | ||||||
| Live with a partner | 29415 | 62.8 | 24328 | 60.8 | 32568 | 60.7 |
| Live alone | 12011 | 37.2 | 9643 | 39.2 | 14556 | 39.3 |
| Smoking status | ||||||
| Daily smoker | 8389 | 19.7 | 5229 | 15.5 | 7376 | 16.0 |
| Occasional smoker | 2175 | 5.7 | 1759 | 6.1 | 2962 | 7.3 |
| Ex-smoker | 14810 | 28.9 | 12772 | 29.4 | 17452 | 29.0 |
| Never smoker | 20926 | 45.7 | 18139 | 49.0 | 24619 | 47.6 |
| Perceived stress (PSS-10) | ||||||
| Low/medium stress | 37200 | 77.9 | 31074 | 79.4 | 40625 | 74.5 |
| High stress | 9100 | 22.1 | 6825 | 20.6 | 11784 | 25.5 |
| Alcohol consumption | ||||||
| As recommended | 39308 | 87.1 | 32948 | 90.2 | 46469 | 91.6 |
| Above recommendation | 5690 | 12.9 | 3640 | 9.8 | 4284 | 8.4 |
| Loneliness | ||||||
| Not lonely | . | . | . | . | 48676 | 91.8 |
| Lonely | . | . | . | . | 3215 | 8.25 |
In adjusted analyses, we investigated the temporal changes in citizens’ reporting of perceived high stress level. We found a significant increase over time (OR=1.25; 95% CI: 1.20–1.30) for 2017 compared to 2010 (p<0.0001). The increase did not differ between men and women (p=0.680) and there was no significant difference in temporal development between the four smoking status groups (p=0.055).
In logistic regression models, we investigated the association between smoking status and perceived high stress level. Analyses showed a significant interaction between smoking and sex (p<0.0001 adjusted for age, p=0.0005 fully adjusted) and results are therefore shown by sex (Table 2). We found a significant association between smoking status and perceived high stress level, except that there was no significant difference between ex-smoking and never smoking women. Adjusted odds ratio for daily smoking men was 2.16 (95% CI: 1.93–2.41) compared to never smoking men. Similar results but less pronounced were seen among women. Also, for both sexes, we found that never smokers had the lowest probability of reporting perceived high stress level, followed by ex-smokers and occasional smokers. Daily smokers had the highest probability. In the fully adjusted models, odds ratios decreased, especially for daily smokers. Daily smoking men had 69% higher odds of reporting perceived high stress level and daily smoking women had 36% higher odds, than never smokers of same sex.
Table 2
Smokers’ and non-smokers’ probability of having a high stress level, by sex, 2017
| Characteristics | High stress level (N=52409) (adjusted for age, sex) | High stress level (N=48508) (fully adjusted*) | ||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Men | ||||
| Never smokers | 1 | 1 | ||
| Ex-smokers | 1.43 | 1.29–1.57 | 1.34 | 1.21–1.49 |
| Occasional smokers | 1.37 | 1.17–1.61 | 1.38 | 1.15–1.64 |
| Daily smokers | 2.16 | 1.93–2.41 | 1.69 | 1.50–1.91 |
| Women | ||||
| Never smokers | 1 | 1 | ||
| Ex-smokers | 1.06 | 0.99–1.14 | 1.03 | 0.95–1.12 |
| Occasional smokers | 1.34 | 1.17–1.55 | 1.29 | 1.10–1.51 |
| Daily smokers | 1.78 | 1.62–1.96 | 1.36 | 1.22–1.51 |
Finally, we investigated daily smokers’ tobacco consumption and perceived stress level (Figure 1), based on 7376 observations. We found that when tobacco consumption increased, a higher proportion of persons reported a perceived high stress level. Test for trend was significant (p=0.0004). In all, 40.3% of men and 44.6% of women with a tobacco consumption of 21–26 cigarettes/g tobacco per day had a perceived high stress level.
DISCUSSION
In repeated cross-sectional population-based surveys in the Capital Region of Denmark, we found a significantly increased proportion of citizens with perceived high stress level in 2017 compared with 2010 and 2013. There was no difference in increase in perceived high stress level between smokers and non-smokers. In analyses adjusted for sociodemographic factors, alcohol intake and loneliness, daily smokers had the highest odds of perceived high stress level, followed by occasional smokers and ex-smokers. Never smokers had the lowest odds of perceived high stress level. Furthermore, we found that higher daily tobacco consumption was associated with a higher proportion of citizens with high stress level.
Smoke-free legislation, anti-smoking campaigns and social denormalization of tobacco use are successful tools to combat the devastating health effects of smoking but the social pressure placed on smokers might have negative side-effects. As smokers report that they have perceived the smoke-free legislation to have increased the stigmatization of smoking16, we hypothesized that smokers might have become more stressed over time than non-smokers. This could not be confirmed. To our knowledge, this is the first study to have investigated the temporal changes in stress in smokers and non-smokers, at population level.
The association between smoking and stress is complex. The question about causality remains, but studies indicate that there is a bidirectional association.
Prospective studies indicate that stress in childhood/adolescents is a causal risk factor of smoking initiation. A large cohort study followed children for 16 years and found that girls with high stress at age three had over two times higher odds than girls with low stress to start smoking early16. Another large cohort study showed that low stress resilience in late adolescence increased the risk of smoking in adulthood17. A population-based cross-sectional study, measuring stress with the same tool as our study, found that a one-unit increase in perceived stress was associated with in a significant 5% increased odds of smoking18. Also, those with high stress levels, such as citizens with post-traumatic-stress-disorder (PTSD) have very high smoking rates19 and stress seems to increase smoking desire, in established smokers. Smokers report that stress relief is one of the main reasons for smoking20. Experimental human studies have shown that cigarette craving was increased after stress exposure21,22 and was related to the magnitude of cortisol stress response21. Animal studies confirm that stress during abstinence periods induces self-administration of nicotine intake23. There is a strong socioeconomic gradient in smoking in many countries, and chronic financial stress has been found to partly explain the socioeconomic gradient in smoking24.
Evidence also indicates that perceived stress is a barrier for smoking cessation. Persons with high level of stress (PTSD) have lower odds of quitting25 and in prospective studies of smokers enrolled in a smoking cessation program, stress predicted relapse26.
On the other hand, nicotine abstinences are stressful and nicotine exposure seems to increase stress levels and exacerbate mood disturbances by inducing changes in neural pathways and neurotransmitter systems that are implicated in mood regulation27. A recent review found evidence for smoking being associated with subsequent depression and anxiety and vice versa28.
Finally, studies have studied stress levels after smoking cessation. In our study, we found that ex-smokers had much lower odds of perceived high stress levels than daily smokers, but not as low as never smokers. Previous studies confirm that smoking cessation is associated with decreased, not increased stress29,30, even in highly dependent smokers who reported that smoking helped them cope with stress29. A systematic review, based on 23 studies, concluded that smoking cessation was associated with a decrease in stress levels and an increase in positive mood compared to continuing smoking30. Noteworthy, a study has shown that those who tried to quit smoking but failed had higher odds of stress than those who did not try to quit31.
In our study, we found a dose-response association between smoking intensity and perceived high stress level, which confirms previous findings. A large cross-sectional study showed that increasing levels of perceived stress were significantly associated with heavy smoking among daily smokers18, and a large cohort study found that higher work stress level was associated with greater smoking intensity among smokers32.
Strengths and limitations
The large randomly selected population-based sample, a broad age span, together with use of a weighting procedure ensured a high degree of national generalizability. Measurement of stress was done by use of a validated widely used scale and we adjusted for several potential confounders such as education level, loneliness, and alcohol use.
The study has limitations. First, the most important weakness is the cross-sectional study design, which implies that no conclusions on causality between smoking and stress can be drawn. Second, the chosen stress-scale does not necessarily cover all aspects of stress. A study indicated scalability problems in the current Danish version of PSS-1033. Also, the PSS-10 questionnaire relies on the respondent’s retrospective memory in the last four weeks, imposing a risk of recall bias. Dichotomizing a variable has weaknesses; e.g. a person who just missed the cut-off point of being among the 20% of persons with the highest stress level is classified as not-stressed. Further, data on smoking, alcohol, loneliness and stress are self-reported, so there is risk of information bias. Selection bias cannot be ruled out even though the population weights were included to compensate for non-response.
Smoke-free legislation was implemented in Denmark already in 2007 and since then there has only been a small tightening of the smoke-free environment Act and of other tobacco control Acts. However, many municipalities, workplaces and schools have voluntarily implemented much stronger smoking bans. Further, because of the stagnation of the smoking prevalence in Denmark there has been an increasing public and political focus on smoking, its negative health effects and the need for a stronger tobacco control. We believe, that there has been significantly increased social pressure on smokers from 2010 to 2017.
CONCLUSIONS
In two cross-sectional large population-based studies we found that the proportion of citizens with perceived high stress level had increased over time, but there was no difference in increase between smokers and non-smokers. Daily smokers had the highest odds of perceived high stress level, even when we adjusted for confounders, and a higher daily tobacco consumption was associated with a higher proportion of citizens with perceived high stress level.
Smoke-free legislation, anti-smoking campaigns and social denormalization of tobacco have proven successful in reducing smoking in the population and are important elements of tobacco control. Even though our study did not find that the increase in stress was steeper in smokers than in non-smokers, indicating that the tobacco control strategies have not stressed smokers, we found a worryingly high proportion of daily smokers with perceived high stress level. As a high stress level seems to increase the resistance to quitting and the risk of relapse during a smoking cessation attempt, smoking cessation programs should, to a higher degree, consider implementing stress-coping elements to prevent relapse, especially in heavy smokers. Mindfulness has shown to be a promising intervention to reduce stress and improve cessation outcomes, among smokers with low socioeconomic status34.