
INTRODUCTION
Employees who smoke cigarettes have increased risk of sickness and take more days sick leave from work1; employee smoking may also incur significant costs for their employers2. Smoking employees are more likely to demonstrate productivity loss than their non-smoking co-workers3–5. Comprehensive workplace tobacco policies, including policies regarding a smoke-free campus and buildings, can make it easier for employees to reduce the amount of cigarettes they smoke6,7. Such policies may help change the smoking culture at a workplace and to reduce the number of smoking-related cues on the premises. Smokers may also have to leave the premises to smoke, thereby making it harder to smoke at work. Comprehensive workplace tobacco policies may therefore help lower smoking rates at workplaces8. Such policies would not only reduce costs, but would also help employers contribute to a future smoke-free society.
In the past decades, several national smoke-free policies have been implemented in the Netherlands9. From 1990, smoking was prohibited in public buildings. From 2004, all workers (excluding hospitality industry workers) were entitled to a smoke-free workplace and public transport became smoke-free. In 2008, a partial smoking ban in the hospitality industry was implemented, which was expanded to a full smoking ban in 2014.
Inspired by the Dutch Movement Towards a Smoke-free Generation10, a growing number of public and private outdoor spaces are becoming smoke-free in the Netherlands11. The Movement Towards a Smoke-free Generation was initiated in 2017 by the Dutch Alliance for a Smoke-free Society, a partnership of Lung Foundation Netherlands, the Dutch Heart Foundation, and the Dutch Cancer Society. Its aim is to create a society in which all children born after 2017 are able to grow up smoke-free, and without exposure to tobacco smoke. As a result, a number of settings in which children play and interact have become or are becoming smoke-free, including petting zoos and child day care facilities (by 2020), school grounds (by August 2020), playgrounds (by 2025), and sports grounds (by 2025). In addition, a growing number of hospitals, universities, and private businesses have begun making their campus smoke-free as well12.
Recent research has shown that support for smoke-free policies is on the rise in recent years13–15, with support increasing after the implementation of such policies16–18. A 2016 systematic review of 89 US and Canadian studies showed particularly high levels of support for smoke-free school grounds14. A 2015 systematic review on the support for smoke-free college and university campuses in the US and the UK reported broad support for a smoke-free campus19. A study of college students found an increase of student support from 57.5% to 62.5% two years after implementation20. A similar study among university students reported an increase of average student support from 4.57 up to 5.77, on a 7-point scale, after three years21.
While many studies suggest that support for smoke-free school grounds and campuses increases after implementation14, only a limited number of studies investigated changes in support for smoke-free non-educational campuses, such as workplaces, office premises and industrial areas. One study that measured this explicitly was a US study on a smoke-free worksite policy at a behavioral health institute6. After adopting a comprehensive smoke-free campus policy that prohibited smoking on all indoor and outdoor spaces, support for the policy among employees increased from 60.6% to 80.3% one year after implementation, according to that US study.
In this study, we investigated the change in support for a smoke-free campus among employees before and after implementing a smoke-free campus policy at a healthcare research institute in the Netherlands. The smoke-free policy included a ban on using electronic cigarettes and hookahs.
METHODS
Survey design and sampling
We conducted two surveys among employees to measure the level of support for a smoke-free campus. The campus became smoke-free in January 2019. The first survey was conducted 3 months before (September 2018) and the second one 13 months after (February 2020) implementation of the smoke-free campus policy. The first survey was deliberately conducted well before implementation to allow the institute to use any suggestions made by respondents through the survey for improving the policy. To increase survey uptake, the second survey was conducted in February, thereby avoiding the December/January holiday season. Both surveys included questions about support for the smoke-free campus, as well as demographic questions. Both surveys took about three minutes to complete. In both surveys, an invitation link was sent to all employees via email and through the intranet. Employees knew about the invitation before it was sent, as this study was announced in meetings and through the intranet in the weeks before each survey wave. Due to the strict privacy regulations on handling employee data, employees were only allowed to fill in the surveys anonymously. As we have no data on who filled in both questionnaires, it is not possible to conduct longitudinal analyses.
Study location
The Trimbos Institute22 is a research institute in the Netherlands that conducts research on substance use and mental health including dissemination of information about prevention, treatment, and policy. It develops and conducts mental health and substance abuse prevention, treatment and management programs in the Netherlands and abroad. Founded in 1996 by the merging of two existing research institutes, the Trimbos Institute employs over 200 scientists, health educators and implementation specialists, of which about 25 work in the field of tobacco control.
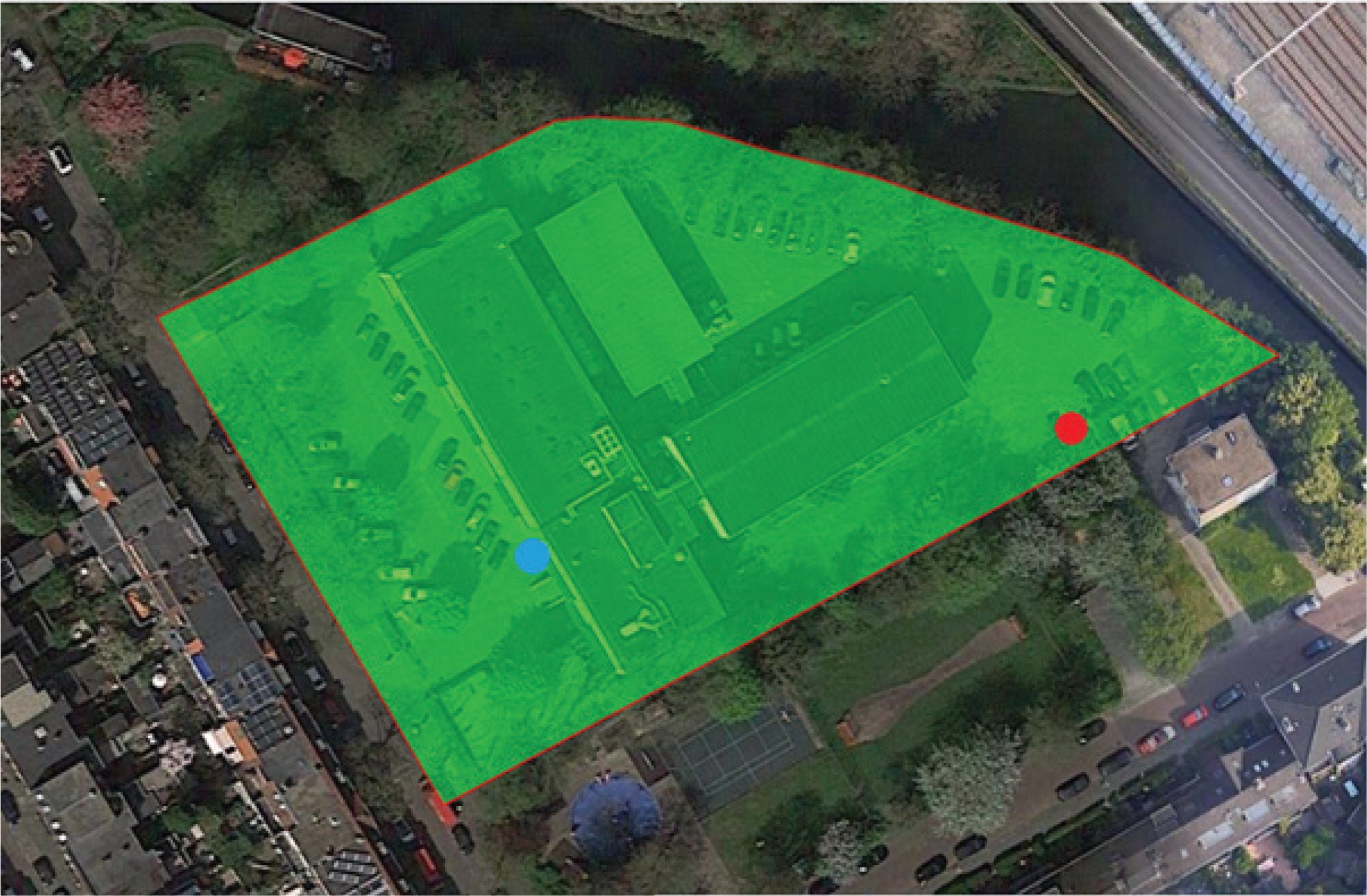
The 7000 m2 campus is situated at the edge of a residential area in Utrecht, the fourth largest city in the Netherlands (with a population of 353000). The campus borders terraced houses, a playground, a canal, and railway tracks. The campus contains one two-story building of 300m2 and two three-story buildings of 570m2 and 950m2. Buildings on the campus house both the Trimbos Institute and six smaller organizations in the field of health sciences (‘tenant organizations’). Until the new policy came into effect, there was a designated smoking area at the back side of the campus (indicated in red in Figure 1).
Creating a smoke-free campus
Although all indoor worksite smoking had been banned by law at the institute since 2004, smoking was still allowed at all outside premises in 2018. All outdoor areas at the Trimbos campus became smoke-free on 1 January 2019.
Nine months before the campus became smoke-free, a committee was set up to coordinate and implement the new policy. This committee consisted of an expert in tobacco control research (MW), a representative of the employee’s council, a communication expert, the head of the human resources department, the head of technical services, and a tobacco control researcher (JB). This committee met with the employee’s council, representatives of the tenant organizations, and the board of directors, to discuss how to make the campus smoke-free. Four months before the campus became smoke-free, the new policy was communicated to all employees via email, intranet posts, employee meetings, and through the survey. Smoking employees who wanted to quit smoking were offered compensation for costs related to smoking cessation. At the time of implementation, smoking cessation support was only partly covered by the universal health insurance scheme in the Netherlands.
On 1 January 2019, the campus became completely smoke-free. That day, the designated smoking area at the back side of the campus was closed and smoking at the campus grounds became prohibited (including using electronic cigarettes and hookahs). The committee placed signs at each entrance, near the former smoking area, and near the bicycle parking shed for employees who bike to work, as is common in the Netherlands. To further communicate the policy to employees, the committee provided flyers in the reception area and in all conference rooms. To inform visitors, they included a reference to the new policy in the email signatures of all employees and a reference to the smoke-free policy in all job advertisements. The city councilor of Utrecht formally re-opened the campus and this event was broadly communicated through the institute’s website and social media channels.
Participants
Participants were employees of the Trimbos Institute. Both employees and interns were included, and we had no inclusion or exclusion criteria. Background characteristics are presented in Table 1. The Central Committee on Research Involving Human Subjects in the Netherlands requires no ethical approval for this non-medical survey research. The study was therefore reviewed and approved by the internal Trimbos Ethics Committee (3050105).
Table 1
Sample characteristics before and after implementation of a smoke-free campus
Questionnaire
The questionnaire was developed by the project committee and the Trimbos communications department.
Analyses
We used SPSS 25 for all analyses. We used a logistic regression to identify predictors of support for a smoke-free campus and perceived importance of having a smoke-free campus. We coded the independent variables as 1 (agree) and 0 (neutral or disagree). The factors included in our model were: time of survey, smoking status, sex, and age. We did not include any additional confounding factors.
RESULTS
Table 1 presents background statistics. We found no significant differences on any of the background variables between surveys. While 129 of 248 employees invited (52.0%) filled in the first survey, 134 of 223 employees (60.1%) filled in the second survey.
Support for a smoke-free campus
Support for the smoke-free campus increased significantly from 64.3% before implementation to 82.1% thirteen months after implementing smoke-free campus policy at the Trimbos Institute (OR=2.55; 95% CI: 1.39–4.70; p=0.003) (Table 2). Smokers and employees aged >55 years were less likely to support a smoke-free campus. Support went from 33.3% to 55.6% among the smokers (n=12 before; n=9 after), from 61.7% to 79.4% among the former smokers (n=60 before; n=63 after), and from 73.7% to 88.7% among the never smokers (n=57 before; n=62 after).
Table 2
Predictors of support for a smoke-free campus among employees of the Trimbos Institute, Utrecht (N=263)
| B | SE B | Wald | p | OR | 95% CI | % | |
|---|---|---|---|---|---|---|---|
| Constant | 1.98 | 0.83 | 5.64 | 0.018* | 7.26 | ||
| Time of survey | |||||||
| Before | - | 64.3 | |||||
| After | 0.94 | 0.31 | 9.12 | 0.003* | 2.55 | 1.39–4.70 | 82.1 |
| Smoking status | |||||||
| Never smoker | - | - | - | 0.020* | 81.5 | ||
| Former smoker | -0.50 | 0.34 | 2.17 | 0.141 | 0.61 | 0.31–1.18 | 70.7 |
| Smoker | -1.55 | 0.57 | 7.49 | 0.006* | 0.21 | 0.07–0.64 | 42.9 |
| Sex | |||||||
| Male | - | 62.5 | |||||
| Female | 0.52 | 0.32 | 2.59 | 0.108 | 1.68 | 0.89–3.17 | 78.0 |
| Age (years) | |||||||
| <26 | - | 5.18 | 0.270 | 92.0 | |||
| 26–35 | -1.29 | 0.81 | 2.55 | 0.110 | 0.27 | 0.06–1.34 | 76.8 |
| 36–45 | -1.22 | 0.84 | 2.10 | 0.147 | 0.30 | 0.06–1.54 | 75.5 |
| 46–55 | -1.51 | 0.82 | 3.41 | 0.065 | 0.22 | 0.04–1.10 | 69.8 |
| >55 | -1.82 | 0.85 | 4.60 | 0.032* | 0.16 | 0.03–0.85 | 61.0 |
Perceived importance of a smoke-free campus
The percentage of employees who believed it is important to have a smoke-free campus significantly increased from 56.6% before implementation to 75.4% thirteen months after implementation (OR=2.28; 95% CI: 1.31–3.97; p=0.004) (Table 3). Smokers were less likely to believe that a smoke-free campus is important. Perceived importance went from 25.0% to 44.4% among the smokers, from 53.3% to 69.8% among the former smokers, and from 66.7% to 85.5% among the never smokers.
Table 3
Predictors of perceived importance of a smoke-free campus among employees of the Trimbos Institute, Utrecht (N=263)
| B | SE B | Wald | p | OR | 95% CI | % | |
|---|---|---|---|---|---|---|---|
| Constant | 0.19 | 0.55 | 0.12 | 0.725 | 1.21 | ||
| Time of survey | |||||||
| Before | - | 56.6 | |||||
| After | 0.82 | 0.28 | 8.43 | 0.004* | 2.28 | 1.31–3.97 | 75.4 |
| Smoking status | |||||||
| Never smoker | - | - | - | 0.001* | 76.5 | ||
| Former smoker | -0.82 | 0.31 | 6.75 | 0.009* | 0.44 | 0.24–0.82 | 61.8 |
| Smoker | -1.79 | 0.54 | 10.85 | 0.001* | 0.17 | 0.06–0.48 | 33.3 |
| Sex | |||||||
| Male | - | 56.9 | |||||
| Female | 0.44 | 0.31 | 2.08 | 0.149 | 1.56 | 0.85–2.85 | 69.9 |
| Age (years) | |||||||
| <26 | - | 2.68 | 0.612 | 64.0 | |||
| 26–35 | 0.45 | 0.52 | 0.74 | 0.389 | 1.57 | 0.56–4.34 | 72.0 |
| 36–45 | 0.53 | 0.56 | 0.87 | 0.350 | 1.70 | 0.56–5.13 | 69.4 |
| 46–55 | 0.05 | 0.53 | 0.01 | 0.923 | 1.05 | 0.37–3.00 | 58.7 |
| >55 | 0.59 | 0.59 | 0.98 | 0.322 | 1.80 | 0.56–5.77 | 65.9 |
DISCUSSION
This study showed that after implementing a smoke-free campus, significantly more employees supported this measure than before the measure was implemented. In addition, more employees came to believe that it is important to have a smoke-free campus. This is in line with other research that shows that support for smoke-free polices increases after implementation14.
Implications for other smoke-free outdoor spaces
In line with previous research6,14,19, we found that initial support for the smoke-free campus was high, and increased in almost all subgroups after implementation. After the policy was implemented, more employees considered a smoke-free campus important. Non-smokers and former smokers were more likely than smokers to support the smoke-free campus, which has also been found also in other studies of smoke-free campus policies23,24.
This research shows that the implementation of a smoke-free campus policy can be a complex process for those involved, especially for those who smoke. Rather than using a strictly top-down approach, it is recommended that a steering group of employees (smokers and non-smokers, managers and staff) work together to develop the policy, address concerns and misconceptions about smoke-free policies, advocate for the policy among peers, provide cessation support, educate staff on the new policy, and evaluate and update the policy as needed25,26. However, as our research shows, these efforts may not be enough to gain complete and full employee support.
In many cases, smoke-free campus policies, such as policies for school grounds, hospital sites, and recreational areas, are not mandated by law. Reasonable arguments for smoke-free spaces can limit the resistance of smokers to these policies27. Research in Spain has shown that protecting children from tobacco smoke exposure is such a reasonable and accepted rationale for smokers and non-smokers for setting smoke-free grounds and campuses28. This argument was also communicated by Trimbos Institute. The institute further communicated that the policy was strongly aligned with its mission, vision, and values, as a healthcare research institute with a strong focus on mental health and addiction and with several researchers working in the field of tobacco control. While the Trimbos Institute borders a playground, the playground is not on the campus and is not visible from all of the grounds; this may have reduced the perceived need to have smoke-free grounds to protect children from tobacco smoke exposure, and consequently influence support for its smoke-free campus policy.
Although the implementation of the smoke-free campus went well, none of the smoking employees accepted the offer of compensation for smoking cessation support. Despite this, the level of compliance to the new smoke-free policy has been very high from the day it was implemented. Conversations with receptionists and members of the general and technical services revealed that all smoking colleagues adhered to the new policy from the beginning. Although there were a handful of non-complying smoking guests, even those guests left the campus quickly after being reminded of the new policy. Overall, the implementation of the new policy was met with near-universal levels of compliance.
While studies have shown that many employees support smoke-free campuses, including smokers, there may remain a group of people who do not support such policies. Despite the clear benefits that smoke-free grounds have for employees and organizations, some view such policies as an infringement on the rights of smokers29, and feel that the benefits of smoke-free outdoor spaces are overstated27. Working with stakeholders to gain support for the policies is a crucial step, but the development and implementation of smoke-free campus policies should not wait for complete support from every patient, student, resident, or employee. As our research shows, support for the policies grows after implementation.
Strengths and limitations
A strength of this study is that we measured support for a smoke-free campus both before and after implementation. This way we were able to investigate the change in support over time, which allowed us to adapt our communication strategy if necessary. A limitation is that we had response rates of 52.0% and 60.6%. While this is comparable to similar studies on smoke-free campuses19, it might have biased the results as people who support a smoke-free campus might have been more likely to respond to the survey invitation. Furthermore, the prevalence of tobacco smoking in this study (9.3% before implementation of the policy) was low compared to the general adult population in the Netherlands (22.2% in 2018)30. Since support for smoke-free policies is generally higher among non-smokers, smoke-free campus policies in organizations with more smoking employees might not experience an equally high level of support. Finally, since we were unable to link pre-implementation and post-implementation survey respondents, we could not take into account staff turnover. Despite that, we did not find significant differences in demographic characteristics among the pre-implementation and post-implementation survey samples.